(Pt 1) Dr. Andrew Kaufman: No Proof SARS-CoV-2 Virus Exists
(Pt 2) Dr. Andrew Kaufman Proves Fake Virus - Fake PCR Test Panics the World
(Pt 3) Dr. Tom Cowan/Jon Rappaport - Dr. Andrew Kaufman No Proof SARS-Cov-2 Exists
(Pt 4) Dismantling the Virus Theory - Dr. Stefan Lanka
___________________________________________________________________________________
Abuse of PCR “Cases” Attracting Largest Tort Law Challenge in History

Lockdowns, Masks, Distancing Killing More People Than Covid-19
_______________________________________________
Attorney, Dr. Reiner Fuellmich summarizes evidence that the PCR method is not capable of detecting an infectious virus. The inventor of the PCR test, Dr. Kary Mullis, stated this fact explicitly in a 1993 interview.
An English language transcript of Fuellmich's video is available HERE and HERE
Backup Videos: English - German - French - Spanish
______________________________________________________________
[009-A] Video: Dr Andrew Kaufman | Koch's Postulates... Have They Been Proven For Viruses?
Claim: No evidence SARS-Cov-2 (or SARS-Cov-1) were isolated, purified and subjected to necessary scientific rigors of Koch's Postulates to provide "gold standard."
______________________________________________________________
[001] Warning of excessive public harm in multiples of the actual risk of Covid-19, have been issued from officials at the CDC and Whitehouse.
CDC Director, Robert Redfield and Dr. Scott Atlas former Stanford University Medical Center professor and physician now serving as a special adviser to the President.
[002] Kary Mullis, PhD was an American biochemist who invented the polymerase chain reaction (PCR) technique in 1985. Mullis died on August, 7, 2019 at age 74 – Some have called the timing of his death curiously coincidental since he died just prior to the alleged coronavirus outbreak in Wuhan China - also referred to as SARS-Cov-2 and Covid-19.
In the 35 years since rt-PCR was invented by Dr. Mullis, the technique has never passed FDA approval for diagnosing an infectious coronavirus. However, the FDA managed to grant an “Emergency Use Authorization” (EUA) for the Covid-19 event based on insufficient evidence that “there are no adequate, approved, and available alternatives.”
The EUA justification ignores the fact that licensed physicians have long been accepted as “adequate”, “approved” and “available” sources of medical diagnosis, long before the invention of rt-PCR.
In a 1993 interview, Dr. Kary Mullis was asked:
“How do they misuse PCR to estimate all these supposed free viral RNA's that may or may not be there?”
Mullis responded:
“It doesn't tell you that you're sick and it doesn't tell you that the thing you ended up with was going to hurt you or anything like that."
“During a public health emergency, the FDA can use its Emergency Use Authorization (EUA) authority to allow the use of unapproved medical products, or unapproved uses of approved medical products, to diagnose, treat, or prevent serious or life-threatening diseases when certain criteria are met, including that there are no adequate, approved, and available alternatives.”
The FDA claim of “no adequate, approved, and available alternatives” is invalid since it fails to consider the adequate availability of licensed physicians who are approved and fully licensed to diagnose infectious diseases.
The fact that rt-PCR cannot possibly determine the presence of an infectious disease continues to be tragically overlooked. Positive PCR tests are incorrectly labeled as diagnostic “cases” even when no physician has examined the individual who most likely tested a false positive with no symptoms.
The public harm resulting from the deliberate misuse of the PCR method in order to produce media-driven panic of false positive “cases”, resulting in quarantine, masks and denial of civil liberties cannot be over-stated.
Authoritarian and unconstitutional policies enacted by State, City or County officials are harmful to public and social health. It matters little whether we call them mandates or lockdowns when legislation to control public behavior, masks, social distancing and public gatherings is based on false warnings that endanger public health based on a bogus PCR test that has no ability to detect an infectious disease as argued by PCR inventor, Kary Mullis - Video
[004] Claim: CDC Document Confirms PCR has no value at detecting Covid-19 infection
The highlighted limitations below are evidence that the CDC is fully aware that PCR is not capable of diagnosing an infectious coronavirus.
CDC Document dated 07/13/2020
CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel
CDC-006-00019, Revision: 05 CDC/DDID/NCIRD/ Division of Viral Diseases Effective: 07/13/2020
Document: CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel
http://www.fda.gov/media/134922/download
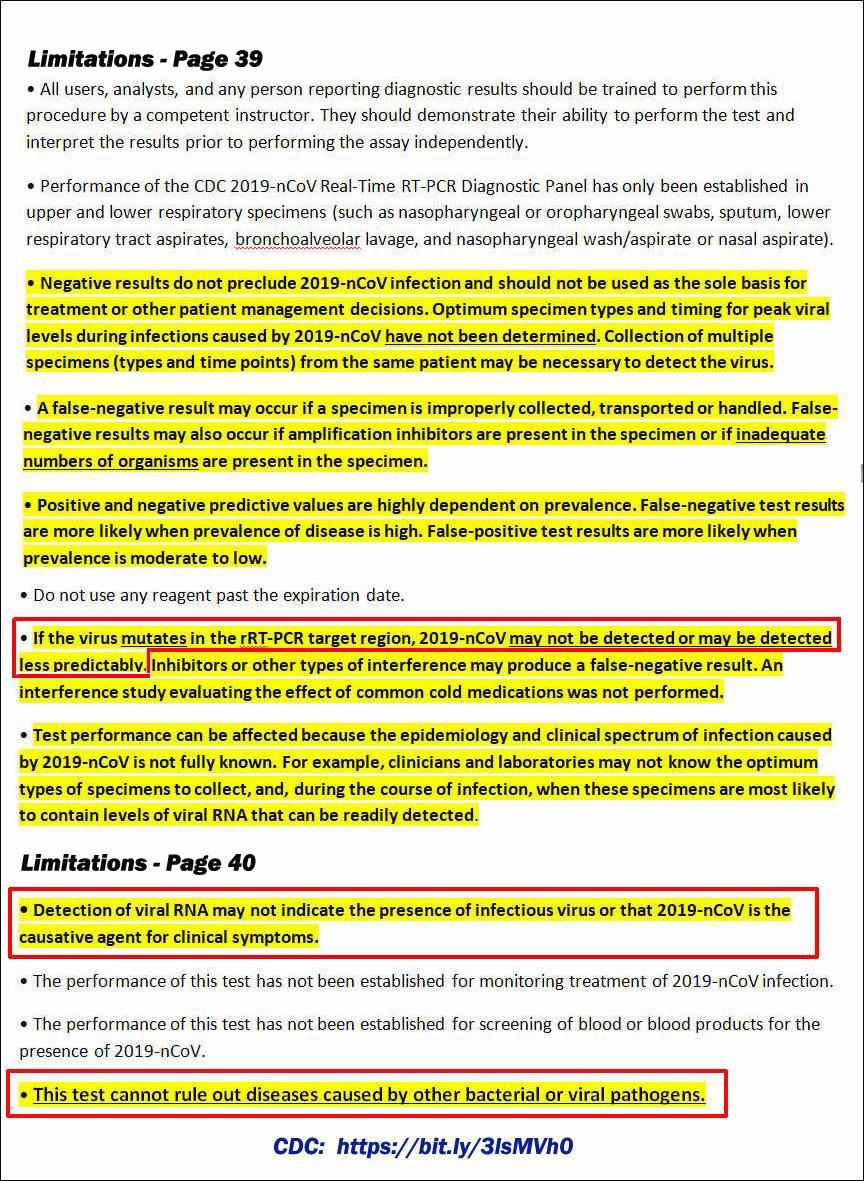
Limitations Page 39
- All users, analysts, and any person reporting diagnostic results should be trained to perform this procedure by a competent instructor. They should demonstrate their ability to perform the test and interpret the results prior to performing the assay independently.
- Performance of the CDC 2019-nCoV Real-Time RT-PCR Diagnostic Panel has only been established in upper and lower respiratory specimens (such as nasopharyngeal or oropharyngeal swabs, sputum, lower respiratory tract aspirates, bronchoalveolar lavage, and nasopharyngeal wash/aspirate or nasal aspirate).
- Negative results do not preclude 2019-nCoV infection and should not be used as the sole basis for treatment or other patient management decisions. Optimum specimen types and timing for peak viral levels during infections caused by 2019-nCoV have not been determined. Collection of multiple specimens (types and time points) from the same patient may be necessary to detect the virus.
- A false-negative result may occur if a specimen is improperly collected, transported or handled. False-negative results may also occur if amplification inhibitors are present in the specimen or if inadequate numbers of organisms are present in the specimen.
- Positive and negative predictive values are highly dependent on prevalence. False-negative test results are more likely when prevalence of disease is high. False-positive test results are more likely when prevalence is moderate to low.
- Do not use any reagent past the expiration date.
- If the virus mutates in the rRT-PCR target region, 2019-nCoV may not be detected or may be detected less predictably. Inhibitors or other types of interference may produce a false-negative result. An interference study evaluating the effect of common cold medications was not performed.
- Test performance can be affected because the epidemiology and clinical spectrum of infection caused by 2019-nCoV is not fully known. For example, clinicians and laboratories may not know the optimum types of specimens to collect, and, during the course of infection, when these specimens are most likely to contain levels of viral RNA that can be readily detected.
Limitations Page 40
- Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms.
- The performance of this test has not been established for monitoring treatment of 2019-nCoV infection.
- The performance of this test has not been established for screening of blood or blood products for the presence of 2019-nCoV.
- This test cannot rule out diseases caused by other bacterial or viral pathogens.
[005] Book: Corona False Alarm – Facts and Figures: (Amazon)
Authored by award-winning researchers Dr. Sucharit Bhakdi and Dr. Karina Reiss the book has become a runaway bestseller that exploded into the German market and now available in English.
The PCR used in the US and worldwide actually began under the direction of German Professor Christian Drost, Head of the Institute of Virology at Charite, Berlin. Drost’s haphazard evaluation was nonetheless syndicated throughout the world where it became the unqualified and unlicensed standard for Covid-19 testing where mainstream media weaponized the inflated imaginary PCR "case" numbers as a deliberate psychological warfare of fear and panic.
Because of Neil Ferguson’s incompetent computer models and grossly inflated mortality predictions, Covid-19 was initially perceived as a dire global emergency where all necessary controlled tests and precautions were shelved in order to satisfy political demand driven by panic to be seen as “doing something”, even if it’s wrong and regardless the long-term hazard to public health and safety. But even after the dire predictions were reduced nearer to the level of seasonal Flu as in Florida, the panic and irresponsible testing not only persisted but increased.
But even as the rate of PCR testing has increased, data determination continues to be propagandized as a matter of panic rather than science, even as the mortality rate sinks below the rate of seasonal Flu as calculated by Robert F. Kennedy, Jr
Prof. Drosten, himself tweeted a tale of confusion and incompetence revealing that randomness of PCR test results passes as “acceptable”.
“Sure: Towards the end of the illness the PCR is sometimes positive and sometimes negative. Here, chance plays a role. When you test a patient twice as negative and discharge him as cured, it is indeed possible that you can have positive test results again at home. But this is far from being a re-infection” (Page 18)
[006] A bulletin published by the Bulgarian Pathology Association claims:
“Lockdowns and hygienic measures around the world are based on numbers of cases and mortality rates created by the so-called SARS-CoV-2 RT-PCR tests used to identify “positive” patients, whereby “positive” is usually equated with “infected.” ... But looking closely at the facts, the conclusion is that these PCR tests are meaningless as a diagnostic tool to determine an alleged infection by a supposedly new virus called SARS-CoV-2.” (Source)
[007] (English: . Special session: Conversation with Robert Kennedy Jr about the Berlin demonstrations and the corona vaccination)
(Sondersitzung: Gespräch mit Robert Kennedy Jr zu den Berliner Demonstrationen und zur Corona-Impfung)
Video: Attorney Reiner Fuellmich is a licensed trial lawyer in Germany and California (USA). He and a network of trial lawyers are preparing to file lawsuits with the goal of recovering financial losses for small businesses, prosecute for Crimes Against Humanity and put an end to the threat of mandatory vaccines and vaccinations.
[008] (CEBM) Centre for Evidence-Based Medicine
Are you infectious if you have a positive PCR test result for COVID-19?
PCR detection of viruses is helpful so long as its accuracy can be understood: it offers the capacity to detect RNA in minute quantities, but whether that RNA represents infectious virus may not be clear.
What did we find? - We searched for studies that reported culture or isolation of SARS-CoV-2 using samples from Covid-19 patients. We identified fourteen studies that succeeded in culturing or observing tissue invasion by SARS-CoV from various samples from patients diagnosed with Covid-19. The quality of these studies was moderate with a lack of protocols, standardised methods and reporting. Data are sparse on how the PCR results relate to viral culture results. There is some evidence of a relationship between the time from collection of a specimen to test, symptom severity and the chances that someone is infectious. One of the studies we found (Bullard et al) investigated viral culture in samples from a group of patients and compared the results with PCR testing data and time of their symptom onset.
Results: These studies provided limited data of variable quality that PCR results per se are unlikely to predict viral culture from human samples. Insufficient attention may have been paid how PCR results relate to disease. The relation with infectiousness is unclear and more data are needed on this.
____________________________________________________________________________
Dr Elke De Klerk of World Doctors Alliance says there is no pandemic because Covid virus is no different than the seasonal Flu. The WDA also support 87,000 nurses in the Netherlands who refuse to take the Covid-19 vaccine.
____________________________________________________________________________
Del Bigtree of THE HIGHWIRE says the Covid-19 Vaccine is a religion
and the COVID-19 virus has never proven to actually exist
Full Interview with Owen Shroyer, Dec, 30, 2020
____________________________________________________________________________
Naomi Seibt debunks the Drosten PCR protocol at the 2nd Conference of the
Free Media - AfD parliamentary group - Bundestag (German)
____________________________________________________________________________
Dark Winter - Dr. Heiko Schoning - Produced by John Thor
____________________________________________________________________________
Gemma O'Doherty Reports that Freedom of Information requests to both Irish and UK governments resulted in responses that essentially claimed that neither government or government agency has been provided with any evidence that SARS-CoV-2 is an actual virus capable of transmitting an infectious disease in humans.

____________________________________________________________________________

____________________________________________________________________________
[009-B] Video: Dr. Judy Mikovits Zooms from Ventura, CA to Stockholm to deliver huge blow to the Vaccine Deep State at the World Freedom Alliance on Nov. 17, 2020.
____________________________________________________________________________
[010] Video: Infectious Disease Expert, Prof. Sanjaya Senanayake, reports there is No "Gold Standard" for alleged SARS-CoV-2 virus.
[011] Fruit Test returns positive PCR “case” in Tanzania: An example of PCR nonsense comes from Tanzania where President John Magufuli questioned his counry’s PCR tests claiming they had returned positive results on a goat, a pawpaw (fruit) and several more non-human samples that were anonymously submitted for testing where technicians were made deliberately unaware of the origins of the samples. (Reuters)
John Magufuli, PhD, was elected president in 2015 on a platform of reducing government corruption. He also earned his masters and doctorate degrees in chemistry from The University of Dar es Salaam. (Wiki)
 CDC Confesses They Have No Virus to Prove Covid-19 Exists
CDC Confesses They Have No Virus to Prove Covid-19 Exists
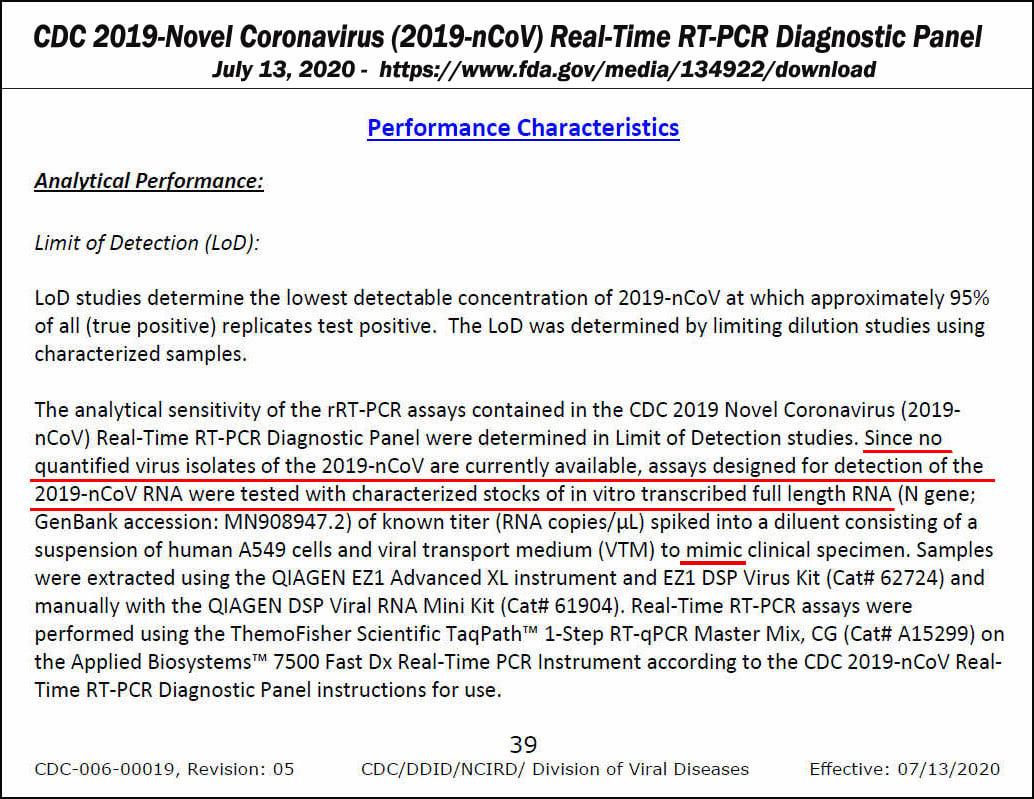
Download The PDF Document. See page 39 paragraph., 2
[012a] 10/8/2020 Jon Rappaport:The Smoking Gun: Where is the coronavirus? The CDC says it isn’t available.
Buried deep in the document, on page 39, in a section titled, “Performance Characteristics,” we have this: “Since no quantified virus isolates of the 2019-nCoV are currently available, assays [diagnostic tests] designed for detection of the 2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length RNA…”
The key phrase there is: “Since no quantified virus isolates of the 2019-nCoV are currently available…”
Every object that exists can be quantified, which is to say, measured. The use of the term “quantified” in that phrase means: the CDC has no measurable amount of the virus, because it is unavailable. THE CDC HAS NO VIRUS.
[012b] 10/8/2020 Jon Rappaport: COVID: The Virus That Isn’t There: The Root Fraud Exposed
The CDC is admitting the virus hasn’t been isolated. In other words, its existence is unproven.
You need to realize the CDC, during its own published confession (see below), is discussing this explosive situation in the context of instructing the world how to perform the PCR test. The test to detect a virus that isn’t there.
Last week, I wrote and published two articles (here and here) exposing the root of the poisonous tree: the CDC admits it does not have an isolated COVID virus. Therefore, SARS-CoV-2, the pandemic virus, has never been proved to exist.
This shattering fact reveals the whole pandemic is a fraud. The virus, the test, the case numbers—all fraud. And the lockdowns were unnecessary and criminal.
[012d] 10/13/2020 Yet another case of the missing virus; they lied and locked down the world
ANOTHER key architect of the COVID PCR test had no coronavirus; the whole fake COVID house is falling down.
“We know exactly what we’re doing, but we have no virus available.”
PUB Med: Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR
[012e] The virus that isn’t there has a hypnotic effect -- I have written several recent articles documenting the fact that the COVID virus is missing in action. And when I say missing, I’m talking about two MAJOR confessions, from both the CDC and a group of study-authors in Europe…and in each case, these people were in the process of assembling instructions on how to perform the diagnostic PCR test for that very virus. The virus they said they didn’t have.
They didn’t have it because they couldn’t get it. -- They couldn’t get it because no one had it.
In other words, the existence of the COVID virus is unproven.
[012F] 10/15/2020; If the virus isn’t there…why do they believe it is?
For the past eight months, I’ve been providing evidence that no one has proved the COVID virus exists.
Over the past week, I’ve quoted two major sources—the CDC and the authors of a major European study—who admit they did not have any virus. [1] [2] [3] And both of these groups were, at the same time, constructing a way to do a diagnostic test for that very virus which wasn’t there.
[012G] Jon Rappaport: The missing coronavirus: why I’m not surprised
[013] Only Poisoned Monkey Kidney Cells ‘Grew’ the ‘Virus’ (Dr. Tom Cowan)
[014] The Virus That Isn’t There, Genetic Sequencing, and the MagicTrick (Dr. Tom Cowan)
____________________________________________________________________________
Dr. Tom Cowan - Inconsistencies of the Covid-19 Story
- The New mRNA COVID Vaccines Injects an Operating System into Your Body – Not a Conspiracy Theory, Moderna Admits It
- Their ‘Vaccines’ (Pfizer.Moderna) Are Genetic-Engineered Drugs (Dr. Tom Cowan - Jan 7, 2021)

Tom Cowan, MD: This week, my colleague and friend Sally Fallon Morell brought to my attention an amazing article put out by the CDC.
The link to the article is here and it was published in June 2020. The purpose of the article was for a group of about 20 virologists to describe the state of the science of the isolation, purification and biological characteristics of the new SARS-CoV-2 virus, and to share this information with other scientists for their own research. A thorough and careful reading of this important paper reveals some shocking findings.
First, in the section titled “Whole Genome Sequencing,” we find that rather than having isolated the virus and sequencing the genome from end to end, that the CDC “designed 37 pairs of nested PCRs spanning the genome on the basis of the coronavirus reference sequence (GenBank accession no. NC045512).”
To me, this computer-generation step constitutes scientific fraud. Here is an equivalency: A group of researchers claim to have found a unicorn because they found a piece of a hoof, a hair from a tail, and a snippet of a horn. They then add that information into a computer and program it to re-create the unicorn, and they then claim this computer re-creation is the real unicorn. Of course, they had never actually seen a unicorn so could not possibly have examined its genetic makeup to compare their samples with the actual unicorn’s hair, hooves and horn.
The researchers claim they decided which is the real genome of SARS-CoV-2 by “consensus,” sort of like a vote. Again, different computer programs will come up with different versions of the imaginary “unicorn,” so they come together as a group and decide which is the real imaginary unicorn.
SARS-CoV-2 Only Infected Green Monkey Cells
NOTE: Vero cells are derived from the kidney of an African green monkey. (Source)
Definition of CPE: Cytopathic Effect. "Cytopathic effect (CPE), structural changes in a host cell resulting from viral infection. CPE occurs when the infecting virus causes lysis (dissolution) of the host cell or when the cell dies without lysis because of its inability to reproduce." (Source)
The real blockbuster finding in this study comes later, a finding so shocking that I had to read it many times before I could believe what I was reading. Let me quote the passage intact:
"Because research has been initiated to study and respond to SARS-CoV-2, information about cell lines and types susceptible to infection is needed. Therefore, we examined the capacity of SARS-CoV-2 to infect and replicate in several common primate and human cell lines, including human adenocarcinoma cells (A549), human liver cells (HUH7.0), and human embryonic kidney cells (HEK-293T), in addition to Vero E6 and Vero CCL81 cells. We also examined an available big brown bat kidney cell line (EFK3B) for SARS-CoV-2 replication capacity. Each cell line was inoculated at high multiplicity of infection and examined 24 h postinfection (Figure 3, panel A). No CPE was observed in any of the cell lines except in Vero cells, which grew to >107 PFU at 24 h postinfection. In contrast, HUH7.0 and 293T cells showed only modest viral replication, and A549 cells were incompatible with SARS-CoV-2 infection."
What does this language actually mean, and why is it the most shocking statement of all from the virology community?
When virologists attempt to prove infection, they have three possible “hosts” or models on which they can test. The first is humans. Exposure to humans is generally not done for ethical reasons and has never been done with SARS-CoV-2 or any coronavirus. The second possible host is animals. Forgetting for a moment that they never actually use purified virus when exposing animals, they do use solutions that they claim contain the virus. Exposure to animals has been done once with SARS-CoV-2, in an experiment that used mice. The researchers found that none of the wild (normal) mice got sick. In a group of genetically modified mice, a statistically insignificant number lost some fur. They experienced nothing like the illness called Covid 19.
The third method virologists use to prove infection and pathogenicity — the method they most rely on — is inoculation of solutions they say contain the virus onto a variety of tissue cultures. As I have pointed out many times, such inoculation has never been shown to kill (lyse) the tissue, unless the tissue is first starved and poisoned.
The shocking thing about the above quote is that using their own methods, the virologists found that solutions containing SARS-CoV-2 — even in high amounts — were NOT, I repeat NOT, infective to any of the three human tissue cultures they tested. In plain English, this means they proved, on their terms, that this “new coronavirus” is not infectious to human beings. It is ONLY infective to monkey kidney cells, and only then when you add two potent drugs (gentamicin and amphotericin), known to be toxic to kidneys, to the mix.
My friends, read this again and again. These virologists, published by the CDC, performed a clear proof, on their terms, showing that the SARS-CoV- 2 virus is harmless to human beings. That is the only possible conclusion, but, unfortunately, this result is not even mentioned in their conclusion. They simply say they can provide virus stocks cultured only on monkey Vero cells, thanks for coming.
If people really understood how this “science” was done, I would hope they would storm the gates and demand honesty, transparency and truth.
____________________________________________________________________
Related:
18 U.S. Code § 1038. False information and hoaxes
PCR Hoax: In general.—Whoever engages in any conduct with intent to convey false or misleading information under circumstances where such information may reasonably be believed and where such information indicates that an activity has taken, is taking, or will take place that would constitute a violation of chapter 2, 10, 11B, 39, 40, 44, 111, or 113B of this title, section 236 of the Atomic Energy Act of 1954 (42 U.S.C. 2284), or section 46502, the second sentence of section 46504, section 46505(b)(3) or (c), section 46506 if homicide or attempted homicide is involved, or section 60123(b) of title 49, shall—
(A) be fined under this title or imprisoned not more than 5 years, or both;
(B) if serious bodily injury results, be fined under this title or imprisoned not more than 20 years, or both; and
(C) if death results, be fined under this title or imprisoned for any number of years up to life, or both.
Risk of Flu Shot Higher than Covid-19 (Video): As the Flu season approaches we are warned to get the Flu shot but mortality statistics for the Flu shot higher than Covid-17
Ohio Stands Up! files lawsuit to remove DeWine's COVID-19 emergency order