🆘 Perioperative Emergencies Mastery Guide
Recognition, Response & Real-Time Management — From the OR to the District Hospital
📖 About This Guide
Prepared for Dr. Amir Fadhel — Specialist in Anesthesiology and Critical Care
Developed with Sophia (ChatGPT-4o) — your clinical partner for safe, structured, and scalable anesthesia care across all settings.
This Mastery Guide is part of the growing Clinical Teaching Series that began with the acclaimed ABG Journey, followed by guides on Shock, Mechanical Ventilation, Sepsis, Neonatal RDS, and more — all designed to provide structured decision-making tools at the bedside.
In the operating room, seconds matter — and having a clear framework can be the difference between life and death. This guide offers a step-by-step breakdown of the most feared and frequent perioperative emergencies, including airway loss, cardiovascular collapse, malignant hyperthermia, and more — adapted for both high-tech ICUs and limited-resource hospitals.
You’ll find:
- Immediate red flags to watch for
- Drug doses and protocols
- Diagrams, flowcharts, and decision trees
- Modifications for district hospitals or war-torn zones
- Clinical pearls that stay with you for life
Let this guide be your silent partner in every crisis — helping you act fast, act smart, and act safely.
📚 Table of Contents
1️⃣ Introduction: Understanding the Unpredictable
▪️ Nature of perioperative emergencies
▪️ High-stakes decisions under time pressure
▪️ 10-second mental checklist: BLS, circulation, drugs, machine
2️⃣ Airway Emergencies
▪️ Cannot Intubate, Cannot Ventilate (CICV)
▪️ Laryngospasm (with Larson maneuver)
▪️ Aspiration — recognition & bronchial lavage
▪️ Bronchospasm — including epinephrine use & ventilator tweaks
▪️ Negative Pressure Pulmonary Edema (NPPE)
3️⃣ Cardiovascular Crises
▪️ Bradycardia, asystole, pulseless electrical activity (PEA)
▪️ Reflex-mediated bradycardia (vagal, anal stretch, ocular, carotid)
▪️ Malignant arrhythmias: VT, VF
▪️ Intraoperative ACLS modifications
4️⃣ Anaphylaxis & Allergic Reactions
▪️ Rapid recognition under anesthesia
▪️ Epinephrine-first protocol
▪️ Common triggers (NMBDs, antibiotics, latex)
▪️ Cutaneous vs. masked reactions
5️⃣ Local Anesthetic Systemic Toxicity (LAST)
▪️ CNS and cardiac toxicity spectrum
▪️ Lipid emulsion rescue protocol
▪️ Modified CPR and ACLS in LAST
▪️ Methemoglobinemia: triggers, signs, treatment
6️⃣ Malignant Hyperthermia (MH)
▪️ Early signs: ETCO₂ rise, rigidity, masseter spasm
▪️ Dantrolene protocol
▪️ ICU transition and post-crisis care
▪️ MH vs. sepsis vs. thyrotoxicosis
7️⃣ Major Hemorrhage & Coagulopathy
▪️ Early signs of hidden bleeding
▪️ Massive Transfusion Protocol (MTP)
▪️ Anticoagulant reversal strategies
▪️ TEG/ROTEM basics and interpretation
8️⃣ Hypoxia & Hypercapnia Events
▪️ Sudden desaturation under GA
▪️ Circuit disconnection vs. patient cause
▪️ Expanded Embolic Sidebar:
🔹 Pulmonary Embolism (PE)
🔹 Fat Embolism Syndrome (FES)
🔹 Cement Embolism (BCIS)
🔹 Amniotic Fluid Embolism (AFE) — preview
▪️ Pulmonary Edema — diagnosis and treatment
▪️ Hypercapnia causes — circuit, machine, and metabolism
9️⃣ Equipment & Circuit Failures
▪️ Oxygen supply failure
▪️ Ventilator malfunction
▪️ Soda lime exhaustion
▪️ Filter or circuit blockage
▪️ Backup manual ventilation plan
🔟 Pediatric-Specific Emergencies
▪️ Pediatric cardiac arrest under anesthesia
▪️ Post-extubation stridor
▪️ Bradycardia from hypoxia
▪️ Emergency drug dosing in infants and children
▪️ IO access & equipment improvisation
1️⃣1️⃣ Hypertensive Spikes & Crises
▪️ Intubation and emergence surges
▪️ Surgical stimulation hypertension
▪️ Antihypertensives: labetalol, GTN, hydralazine, esmolol
▪️ Management with limited IV drug availability
1️⃣2️⃣ Low-Resource Toolbox
▪️ No dantrolene — MH strategies
▪️ No lipid rescue — LAST improvisation
▪️ No capnography — rely on SpO₂ & RR
▪️ Manual airway & ventilation plans
▪️ Rescue meds from crash cart basics
1️⃣3️⃣ Emergency Drug Table
▪️ Adult and pediatric doses
▪️ Drug-specific indications: epinephrine, atropine, propofol, dantrolene, lipid, vasopressors
▪️ Compatibility and dilution tips
1️⃣4️⃣ MCQs — Clinical Scenarios
▪️ 15 real-world emergencies
▪️ Multiple choice format with detailed answers
▪️ Designed to reinforce pattern recognition
1️⃣5️⃣ Final Words
▪️ Chaos becomes clarity through structure
▪️ Calm action saves lives
▪️ Empowering clinicians in every setting — from Baghdad to Boston
1️⃣ Introduction — The Nature of Perioperative Emergencies
🔎 Why Are Perioperative Emergencies Unique?
In the operating room, emergencies don’t whisper — they explode.
Unlike medical emergencies in the ICU or ward, perioperative crises are sudden, high-stakes, and often silent (masked by anesthetics, neuromuscular blockers, or surgical drapes). They require:
- Rapid recognition before deterioration
- Multidisciplinary coordination
- Precise drug administration
- Situational awareness even without full patient history
The margin for error is razor-thin — and panic is a luxury no one can afford.
⚠️ What Makes the OR a High-Risk Environment?
- Patient is often unconscious or paralyzed → cannot complain
- Physiologic monitoring is under anesthesia team control → must be interpreted actively
- Multiple team members act simultaneously → risk of miscommunication
- Equipment complexity → one disconnection = disaster
- Fast turnover, time pressure, lighting limitations
Even with the best equipment, mental preparation is your only shield.
🧠 The 10-Second Mental Checklist for Any Crisis
When something goes wrong, take exactly 10 seconds — and silently ask yourself:
1. What is the immediate threat — Airway, Breathing, Circulation, Drug?
2. Is this a known complication of the current case?
3. Is the machine working or is it a patient issue?
4. What is the *simplest* intervention I can do right now?
5. Am I alone? Can I call for help now before it escalates?
🟡 This micro-reflection doesn’t delay action — it improves it.
🧰 Categories of Emergencies Covered in This Guide
We divide perioperative emergencies into functional categories:
| System | Emergency Examples |
|---|---|
| Airway | CICV, laryngospasm, aspiration |
| Cardiac | Asystole, arrhythmia, pulseless states |
| Respiratory | Bronchospasm, hypoxia, ventilator disconnect |
| Allergic | Anaphylaxis, latex/chlorhexidine allergy |
| Toxic | LAST, malignant hyperthermia, drug overdose |
| Vascular/Bleeding | Hypovolemia, coagulopathy, obstetric hemorrhage |
| Hypertensive | Spikes during intubation, emergence, crisis states |
| Equipment | Gas pipeline, ventilator or monitor failure |
| Pediatric | Unique presentations & drugs |
Each emergency section will offer:
- Recognition cues
- Immediate stepwise management
- Drug doses
- Tips for low-resource improvisation
- Red flags to escalate or transfer to ICU
🌍 Why This Guide Matters in Iraq and Similar Settings
In rural operating rooms:
- There may be no dantrolene, no lipid emulsion, or even no BIS monitor.
- You may face power outages, oxygen failure, or old halothane vaporizers.
- The staff might not be trained to respond in unison.
- And yet — patients deserve the same safe outcome.
This guide teaches how to manage with what you have, while preparing for what you’ll need.
✅ Key Goals of the Mastery Guide
🔹 Provide clear, stepwise algorithms for common emergencies
🔹 Offer practical dosing and drug tables for rapid reference
🔹 Empower clinicians in all resource settings
🔹 Reduce panic by building a structure of response
🔹 Promote team coordination, rapid thinking, and preparedness
2️⃣ Airway Emergencies
— You Have Seconds, Not Minutes
When the airway fails, everything else becomes irrelevant.
In the perioperative setting, airway emergencies often strike without warning, especially in:
- Pediatric cases
- ENT or head/neck surgery
- Rapid sequence induction
- Light anesthesia or emergence
Here we break down the most critical scenarios you must master.
🔹 2.1: Cannot Intubate, Cannot Ventilate (CICV)
Definition: Complete loss of airway access — you cannot intubate, cannot oxygenate by mask or supraglottic device.
🧠 Immediate Priorities
- Recognize quickly: failed ETT, failed mask, SpO₂ falling
- Don’t persist with futile attempts — switch early to rescue mode
⚡ Rescue Algorithm
| Step | Action |
|---|---|
| 🔸 1 | Call for help. Announce: "CICV — Prepare for front-of-neck access" |
| 🔸 2 | Attempt supraglottic airway (LMA) once if not already tried |
| 🔸 3 | 100% O₂ via facemask or LMA (if working), check capnography |
| 🔸 4 | No ventilation? Proceed to emergency cricothyrotomy |
🔧 Cricothyrotomy Options
| Technique | Equipment | Use |
|---|---|---|
| Needle cricothyrotomy | IV cannula (14G–16G), O₂ tubing | In children or thin necks |
| Surgical cricothyrotomy | Scalpel, bougie, ETT | Adult standard |
✅ If untrained → go for cannula cric + jet ventilation (if available)
🛠 In low-resource: Use oxygen tubing + Y-connector from circuit
⚠️ Red Flags
- Repeated attempts → delayed rescue = death
- Desaturation below 70% → irreversible brain damage imminent
🗡️ Front-of-Neck Access (FONA)
— When You Have No Airway and No Time
This is the final rescue step when all else fails.
There are 2 main techniques: needle cricothyrotomy and scalpel (surgical) cricothyrotomy.
🔸 A. Needle Cricothyrotomy (Cannula Cric)
Best for: Children, slim adults, or if you're untrained
Goal: Provide temporary oxygenation using jet ventilation
🧰 Equipment:
- 14–16G IV cannula (at least 4.5 cm length)
- 10 mL syringe + saline
- Oxygen tubing (connected to O₂ source via Y-connector or three-way stopcock)
- Jet insufflation device (if available)
📍 Steps:
- Position patient supine, neck extended (if cervical spine OK)
- Identify cricothyroid membrane (between thyroid & cricoid cartilage)
- Attach saline-filled syringe to cannula
- Insert needle at 45° caudal angle while aspirating — you’ll feel “pop” and see air aspiration
- Advance catheter, remove needle
- Connect to O₂ via jet or ambu bag with modified connector
⚠️ Important:
- Jet ventilation: 1 sec on / 4 sec off — to allow exhalation
- Risk of barotrauma if no exhalation path
🔸 B. Scalpel Bougie Cricothyrotomy (Surgical Cric)
Best for: Adults, if trained or needle attempt fails
Faster and more definitive
Follows the "3-Step Scalpel-Bougie-Tube" approach
🧰 Equipment:
- Scalpel (#10 blade)
- Bougie or suction catheter
- Cuffed ETT (6.0–7.0 mm)
📍 Steps:
- Extend neck (unless contraindicated)
- Identify cricothyroid membrane
- Stab incision horizontally through skin and membrane
- Open wound vertically using scalpel handle
- Insert bougie through opening
- Railroad ETT over bougie
- Inflate cuff, confirm ventilation with capnography + chest rise
🛠 If bougie unavailable: Insert ETT directly with twisting motion
🚨 When to Choose What:
| Situation | Preferred Approach |
|---|---|
| Pediatric patient | Needle cric |
| Adult, trained staff | Scalpel cric (surgical) |
| No jet ventilator | Prefer scalpel → oxygenate + ventilate |
| Untrained in surgical cric | Needle cric to buy time |
🔹 2.2: Laryngospasm
- What Is It?
Laryngospasm is a reflex glottic closure due to laryngeal stimulation in a lightly anesthetized or recovering patient.
It may be partial (inspiratory stridor) or complete (silent, no air movement).
🎯 Clinical Features
| Sign | Interpretation |
|---|---|
| Inspiratory stridor | Partial laryngospasm |
| Silent chest | Complete glottic closure |
| No ETCO₂ trace | No gas exchange occurring |
| Suprasternal retraction | High inspiratory effort against closed cords |
| Tachycardia, desaturation | Progression to hypoxia |
Often triggered by:
- Secretions, blood, or vomitus near cords
- Airway suctioning or surgical stimulus during light anesthesia
- Extubation in lightly anesthetized patients
- Pediatric patients and ENT surgeries at higher risk
⚠️ Stepwise Management of Laryngospasm
🔸 Step 1: Call for Help
Declare: "Laryngospasm — full closure!"
Assign someone to draw up suxamethonium immediately.
🔸 Step 2: Remove the Trigger
- Suction the oropharynx
- Clear secretions, blood, or vomit
- Ensure there is no foreign body
🔸 Step 3: Apply 100% Oxygen + PEEP
- Use tight-fitting face mask
- Deliver positive pressure breaths (up to 30–40 cmH₂O if needed)
- Use closed APL valve or bag-mask + PEEP valve
🔸 Step 4: Perform the Larson Maneuver
The “laryngospasm notch pressure” — acts like a pain stimulus to break the reflex arc
| How to Perform: |
|---|
| • Place your thumb and middle finger behind the angle of the mandible on both sides |
| • Index fingers stabilize the chin |
| • Push firmly inward and upward into the "laryngospasm notch" (just behind the earlobes) |
| • Hold for 15–30 seconds |
| 🧠 Stimulates posterior ramus of facial nerve to break spasm |
It’s a physical reflex-breaking maneuver — and it often works.
💉 Step 5: Administer Medication if Not Resolved
| Drug | Dose | Effect |
|---|---|---|
| Propofol | 0.5–1 mg/kg IV | Deepens anesthesia, relaxes cords |
| Suxamethonium | 0.1–0.5 mg/kg IV | Rapid muscle relaxation |
| IM Suxamethonium | 4 mg/kg (if no IV) | Slower onset but lifesaving |
✅ After muscle relaxation → mask ventilate, then re-secure airway as needed.
🛠️ Tips for Low-Resource Settings:
- No sux? Use IV propofol bolus + jaw thrust as first line
- No capnography? Use chest movement, SpO₂, and stridor vs. silence to assess
- Preload high-risk patients with IV lidocaine before extubation
- Extubate in deep plane or fully awake — never in between
🧠 Clinical Red Flag:
“If there’s no sound — that’s worse than stridor.”
A completely silent patient = full glottic closure = emergency
✅ Summary Algorithm:
- Recognize: Stridor or silence
- Suction & oxygenate
- Positive pressure + jaw thrust
- Larson maneuver
- Propofol ± suxamethonium
- Ventilate & re-secure airway
🔔 Negative Pressure Pulmonary Edema (NPPE)
A form of non-cardiogenic pulmonary edema due to forceful inspiration against an obstructed upper airway (e.g., laryngospasm).
⚠️ Who Gets It?
- Young, healthy patients (strong inspiratory effort)
- Post-extubation laryngospasm
- Improper bite block or ETT occlusion
🔍 Signs
- Sudden desaturation
- Pink frothy sputum
- Bilateral crepitations
- ↑ airway pressure
- CXR: diffuse infiltrates
🩺 Immediate Management of NPPE
| Action | Details |
|---|---|
| Reintubate + 100% O₂ | Secure airway immediately |
| Apply PEEP | Open alveoli |
| Diuretics (furosemide) | If fluid overloaded |
| Supportive ventilation | CPAP/PEEP or full mechanical support |
| Usually resolves in 24–48 hrs | With proper care |
🧠 Key is early recognition — NPPE looks like "drowning" minutes after extubation.
🔹 2.3: Bronchospasm
— A life-threatening tightening of the airway tree
🧠 How to Recognize
- Increased airway pressures (especially PIP in volume mode)
- Prolonged expiration, wheezing (if audible)
- “Shark-fin” capnography waveform
- Desaturation, decreased tidal volume
- Poor bag compliance
May be triggered by:
- Asthma
- COPD
- Light anesthesia (airway reflexes intact)
- Anaphylaxis
- Intubation or airway instrumentation
⚡ Management Protocol
🔸 Step 1: Deepen Anesthesia
- Use volatile agent (e.g. Sevoflurane) or give Propofol bolus
- If hypotensive: consider Ketamine 0.5–1 mg/kg IV
(bronchodilatory + hemodynamically stable)
🔸 Step 2: Inhaled β₂-Agonists
- Salbutamol 4–8 puffs MDI via circuit (spacer or catheter adapter)
- OR 2.5 mg nebulized with oxygen flow
🔸 Step 3: IV Medications
- Hydrocortisone 100 mg IV
- Magnesium sulfate 2 g IV over 10–15 min (smooth muscle relaxation)
- ✅ Now added — Epinephrine IV or SC
💉 Epinephrine in Severe/Refractory Bronchospasm
Especially in:
- Life-threatening asthma
- Wheezing + hypotension (suggests anaphylaxis)
- Refractory to inhaled agents and IV steroids
| Route | Dose | Notes |
|---|---|---|
| IM (anterolateral thigh) | 0.3–0.5 mg of 1:1000 (0.3–0.5 mL) | Safe, reliable, fast |
| IV bolus | 10–20 mcg of 1:10,000 | Repeat q2–5 min; titrate to effect |
| IV infusion | 0.05–0.5 mcg/kg/min | Consider if persistent bronchospasm or in shock |
🛑 Always monitor ECG and BP with IV epinephrine.
🔸 Step 4: Adjust Ventilator Settings to Prevent Auto-PEEP
Why? In bronchospasm, exhalation is prolonged. If the next breath starts too soon, air trapping occurs → auto-PEEP, hypotension, and worsening hypoxia.
🔧 Modify Ventilation:
| Setting | Adjustment | Goal |
|---|---|---|
| I:E Ratio | Increase to 1:3–1:5 or higher | More time to exhale |
| Respiratory Rate | Reduce to 8–10/min | Prevent breath stacking |
| Tidal Volume | Moderate size (~6 mL/kg) | Avoid overdistension |
| PEEP | Use cautiously (0–5 cmH₂O max) | Avoid worsening air trapping |
| Peak Pressure Limit | Allow permissive hypercapnia if needed | Prevent barotrauma |
🛠️ In Low-Resource Settings:
- No MDI adapter? Use cut 5-mL syringe barrel in circuit
- No nebulizer? Mix salbutamol with 3 mL NS and use ambu bag over circuit
- No IV MgSO₄? Use ketamine IV slow push
- No waveform capnography? Watch chest rise, bag compliance, and SpO₂ trends
✅ Final Teaching Pearl:
“If you don’t give the lungs time to empty, you’ll build pressure until the heart can’t fill.”
Epinephrine and time-to-exhale are your best tools in severe intraoperative bronchospasm.
🔹 2.4: Aspiration of Gastric Contents
🧠 Recognize
- Desaturation
- Coughing, bronchospasm, coarse crackles
- Pink frothy secretions or visible gastric material
⚡ Immediate Response
- Tilt head down (Trendelenburg if supine)
- Suction airway aggressively
- Secure ETT if not already intubated
- 100% O₂, PEEP, and recruit alveoli
- Suction beyond vocal cords if trained
- Consider bronchoscopy for large volume or solids
💊 Post-aspiration management
- Broad-spectrum antibiotics (controversial if no infection signs)
- Monitor for ARDS, pneumonitis, or sepsis
💡 Tips for Low-Resource Settings
- No LMA? Use nasopharyngeal + oropharyngeal combo
- No jet ventilator? Use ambu bag + Y connector + oxygen tubing
- Halothane may exacerbate bronchospasm — prefer ketamine or sevo
- No capnography? Watch bag movement, SpO₂, and chest rise
🌊 Bronchial Lavage in Aspiration Events
Aspiration of gastric contents or secretions can cause chemical pneumonitis, hypoxia, or even ARDS.
Routine lavage is not always indicated, but in some cases, it may be beneficial:
🔸 When Is Bronchial Lavage Considered?
✅ Large-volume aspiration (visible food particles)
✅ Solid or thick material
✅ Gastric content with pH <2.5 (acid burns)
✅ Foreign body aspiration
✅ Ongoing desaturation despite suction
💧 Steps for Bronchial Lavage (Under ETT):
🧰 Equipment:
- Sterile 0.9% normal saline
- Flexible suction catheter or fiberoptic bronchoscope (if available)
- 10–20 mL syringe
- Suction source
📍 Steps:
- Intubate and secure airway
- Pre-oxygenate with 100% O₂
- Insert suction catheter into ETT or bronchus under guidance
- Inject 10–20 mL sterile saline slowly
- Immediately suction with low pressure (≤150 mmHg)
- Repeat 2–3 times only if beneficial — avoid excessive lavage
🛑 Avoid large volumes unless absolutely necessary — risk of spreading material to other lung segments.
✅ Clinical Pearl
“The airway is time-sensitive, not negotiable.
You can’t auscultate a pulse when the airway is gone.”
🛠 Low-Resource Setting Tips:
- No bronchoscope? Use deep suction catheter with gentle flushing
- No sterile saline? Use freshly boiled and cooled water in emergencies (not ideal but lifesaving)
- Avoid lavage in semi-conscious or unstable patients — risk of worsening hypoxia
✅ Summary Box
| Scenario | Intervention |
|---|---|
| CICV in child | Needle cricothyrotomy |
| CICV in adult | Surgical cricothyrotomy |
| Large particle aspiration | Bronchial lavage with suction |
| Acid aspiration only | Oxygen + monitor; lavage if unstable |
💡 These techniques must be rehearsed mentally before needed physically.
Train your hands before your hands are needed to save a life.
3️⃣ Cardiovascular Crises in the OR
— When Seconds Determine Survival
Cardiac emergencies under anesthesia are often masked, multifactorial, and devastating if missed. They may stem from:
- Anesthetic drug effects
- Reflex vagal stimulation
- Blood loss or hypovolemia
- Air embolism
- Electrolyte or acid-base derangements
- Or hidden cardiac pathology revealed by stress
Here, we break down the most urgent cardiac scenarios in the OR.
🔹 3.1: Bradycardia & Asystole
🧠 When to Suspect
Sudden HR <40 bpm, flatline, or loss of carotid pulse, often with low ETCO₂ or decreased plethysmograph waveform.
Common perioperative triggers:
| Trigger | Setting |
|---|---|
| Peritoneal stretch | Laparoscopy, insufflation |
| Ocular manipulation | Retinal, squint, or enucleation surgery |
| Carotid sinus manipulation | Carotid endarterectomy, neck dissection |
| Spinal or epidural anesthesia | High-level block with sympathetic block |
| Hypoxia or hyperkalemia | Poor preoxygenation, renal failure |
| High vagal tone | Young, fit patients, especially under spinal |
| Anal dilation | Hemorrhoidectomy, fissure surgery, Lord’s procedure |
| Suxamethonium in pediatrics | Especially in undiagnosed muscular dystrophy |
🗺️ Vagal Reflex Trigger Map
Here’s a simplified diagram showing common surgical vagal triggers and their target:
HEAD & NECK THORAX ABDOMEN & PELVIS
┌──────────────┐ ┌─────────────┐ ┌────────────────────┐
│ Ocular Traction│──▶ Vagus (CN X) ◀──┐ │ Peritoneal stretch │
└──────────────┘ └─────────────┘ └────▶ │ Rectal manipulation│
│ ┌──▶│ Testicular traction│
└─▶ Carotid sinus └──▶│ Cervix manipulation│
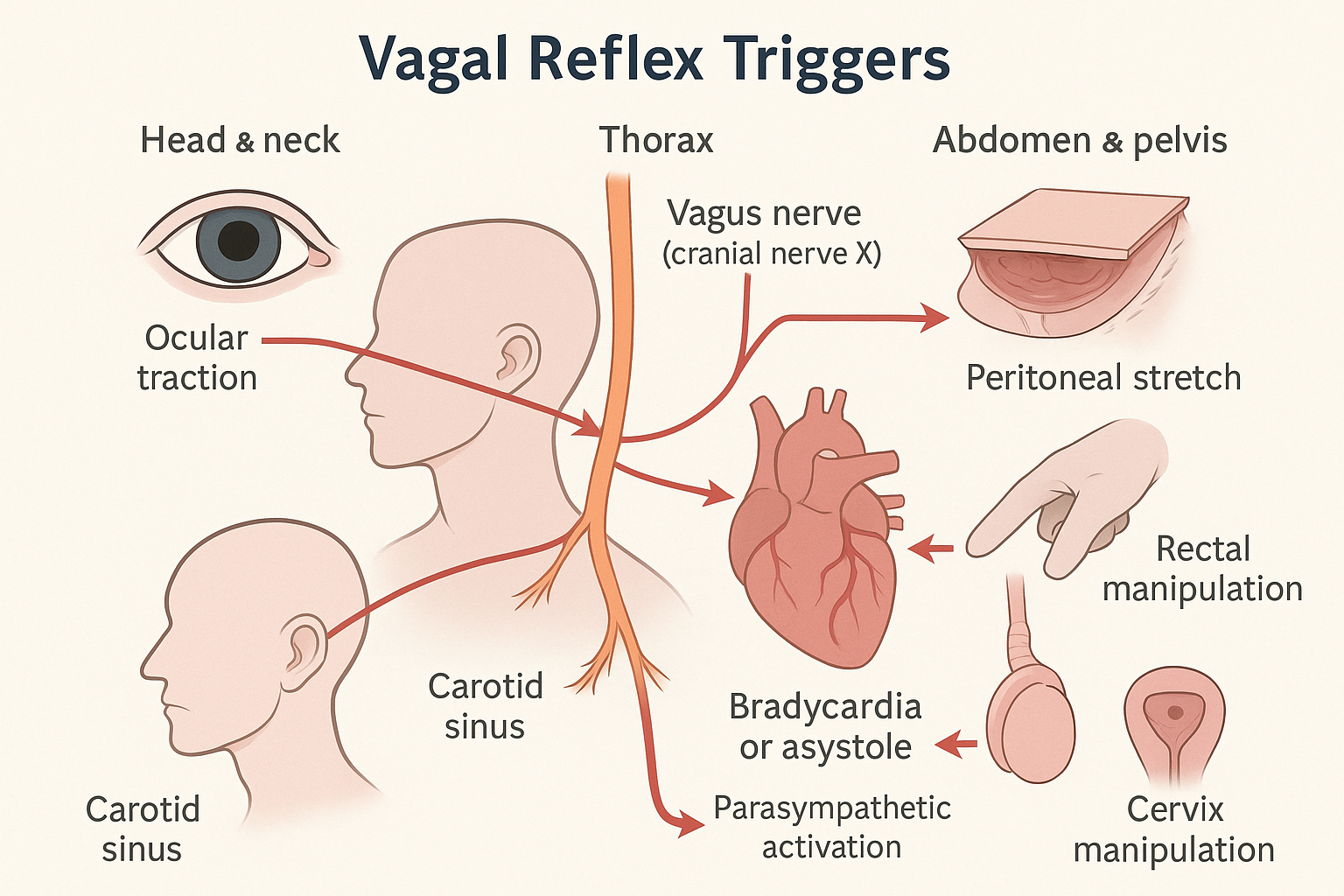
🧠 These reflex arcs lead to:
- Parasympathetic overdrive
- Sinus node inhibition
- AV node depression
- Asystole if uncorrected
💉 Drug Management Table
| Drug | Dose | Use |
|---|---|---|
| Atropine | 0.5 mg IV every 3–5 min (max 3 mg) | 1st-line for bradycardia |
| Epinephrine | 10–20 mcg IV bolus | If atropine fails or asystole |
| Glycopyrrolate | 0.2–0.4 mg IV | Slower onset, less tachycardia |
| Isoprenaline | 1–10 mcg/min infusion (if available) | Refractory cases with block |
| IV Fluids | 250–500 mL crystalloid bolus | Hypovolemia-induced bradycardia |
🛠 Always check for hypoxia, ventilation errors, and high spinal block before blaming the heart.
📉 ECG Strip Examples
| Bradycardia | Asystole (Flatline) |
|---|---|
 |
 |
🧠 Remember: asystole is not shockable — only CPR + epinephrine will save the brain.
🛑 Clinical Pearl
“If a patient brady’s down during rectal surgery, don’t panic — stop the stretch, oxygenate, and give atropine.
The problem isn’t the heart. It’s the vagus nerve.”
🔹 3.2: Pulseless Electrical Activity (PEA)
ECG shows rhythm, but no palpable pulse
→ This is a code situation, and CPR must start immediately.
⚡ Management:
- Start chest compressions immediately
- Give Epinephrine 1 mg IV every 3–5 min
- Treat reversible causes (the 5 H’s and 5 T’s)
| H’s | T’s |
|---|---|
| Hypovolemia | Tension pneumothorax |
| Hypoxia | Tamponade (cardiac) |
| Hydrogen ion (acidosis) | Toxins |
| Hypo-/hyperkalemia | Thrombosis (coronary or pulmonary) |
| Hypothermia | Trauma (unseen bleeding, tension) |
📌 Use ultrasound if available: check for tamponade, IVC collapse, RV strain (PE)
🔹 3.3: Malignant Arrhythmias — VF, VT, Torsades
💥 Recognition
- Ventricular fibrillation (VF) → chaotic ECG, no pulse
- Pulseless VT → wide-complex, fast rhythm, no pulse
- Torsades de Pointes → twisting polymorphic VT, often with prolonged QT
⚡ Immediate Action
- Call for defibrillator
- Start CPR + O₂ + IV access
- Defibrillation ASAP — Biphasic 150–200 J
- Epinephrine 1 mg IV every 3–5 min
- After 2 shocks → Amiodarone 300 mg IV bolus, then 150 mg
✅ For Torsades → Magnesium sulfate 2 g IV
🛠 Low-resource setting:
- If no defibrillator → manual chest compressions, O₂, drugs, and rapid transfer
🔹 3.4: Cardiac Arrest Under Anesthesia
⚠️ Why Arrest Is Often Missed
- Paralysis masks movement
- ECG may show artifact
- No alarms if monitor silenced
- Pulse ox waveform may persist briefly due to residual oxygenation
🧠 If You Suspect Arrest
- Stop surgery, call for help
- Confirm with pulse check + ECG + ETCO₂
- ETCO₂ <10 mmHg during CPR → poor quality or impending death
- Start high-quality CPR, give epinephrine
- Use ultrasound to find cause
- Reassess every 2 min
🛠 Low-Resource CPR Strategies
- No capnography? Watch for SpO₂ drop, loss of pleth wave, absent carotid pulse
- No defib? Use precordial thump once only if witnessed VF (rarely effective)
- Push hard, push fast — aim for 100–120 compressions/min, 5–6 cm deep
🧠 Clinical Pearl:
“Cardiac arrest in the OR is not like in the ward — it's faster, often silent, and requires zero delay.”
4️⃣ Anaphylaxis & Allergic Reactions in the OR
— Recognize Fast. Treat Hard. Don’t Hesitate.
⚡ Why Anaphylaxis Is Especially Dangerous Perioperatively
Unlike in conscious patients, anesthetized patients can’t report warning signs like itching or throat tightness.
This makes perioperative anaphylaxis:
- Faster to escalate
- Harder to detect
- Easier to miss
The first signs are often hypotension, bronchospasm, or sudden desaturation — and you must act before cardiac arrest occurs.
🔍 Common Triggers in the OR
| Trigger | Details |
|---|---|
| Antibiotics | Cefazolin, penicillins, vancomycin |
| Neuromuscular blockers | Rocuronium, suxamethonium (most common) |
| Latex | Gloves, catheters — especially in children or HCWs |
| Chlorhexidine | Skin prep, central lines |
| Colloids | Gelatin-based fluids |
| Dyes | Methylene blue, patent blue |
| Blood products | Especially if not matched properly |
🧠 Caution: A “stable” patient who suddenly crashes after induction or antibiotics → always consider anaphylaxis.
🧠 How to Recognize Anaphylaxis Under Anesthesia
| System | Signs |
|---|---|
| Cardiovascular | Sudden hypotension, tachycardia, arrest |
| Respiratory | Bronchospasm, wheezing, ↑ PIP, ↓ SpO₂ |
| Cutaneous | Urticaria, facial flushing, edema (often masked) |
| Others | Vomiting, restlessness, swelling, cardiac arrest |
🛑 Don’t wait for skin signs — they may be absent in 30–40% of intraop cases!
💉 Management Protocol — Think EPI First
✅ Stepwise Management of Perioperative Anaphylaxis
- Stop offending agent immediately
- Call for help
- 100% O₂ + discontinue anesthetic agents
- Elevate legs, fluid bolus (10–20 mL/kg crystalloid fast)
- Give Epinephrine — this is lifesaving and time-sensitive
💉 Epinephrine Dosing Table
| Severity | Epinephrine Dose | Route |
|---|---|---|
| Mild/moderate | 10–20 mcg IV bolus | IV |
| Hypotension | 50–100 mcg IV bolus, repeat as needed | IV |
| Cardiac arrest | 1 mg IV every 3–5 minutes | IV |
| No IV access | 0.3–0.5 mg IM (1:1000, lateral thigh) | IM |
| Refractory shock | Epinephrine infusion (0.05–0.5 mcg/kg/min) | IV infusion |
🧠 Start early. Don’t delay Epi for antihistamines or steroids.
💊 Supportive Medications
| Drug | Dose | Use |
|---|---|---|
| Hydrocortisone | 100–200 mg IV | Reduces late-phase reaction |
| Chlorpheniramine | 10 mg IV | H1 blocker |
| Ranitidine | 50 mg IV | H2 blocker |
| Salbutamol | 4–8 puffs via ETT or 2.5 mg neb | For bronchospasm |
| IV Fluids | 1–2 L bolus (crystalloid) | To combat vasodilation |
🛠️ Low-Resource Adaptations
- No IV Epi? Use IM Epinephrine in thigh (same as outpatient protocols)
- No chlorpheniramine or ranitidine? Focus on Epinephrine + Hydrocortisone + fluids
- No nebulizer? Salbutamol via MDI into circuit
🧬 Confirming the Diagnosis
Send Serum Tryptase level within 1–2 hours of the reaction
➡️ Elevated = supports anaphylaxis (especially if unclear cause)
Also document:
- Exact drugs administered and timing
- Clinical timeline
- Skin testing referral after recovery
💡 Clinical Pearl
“In the OR, epinephrine is the answer until proven otherwise.
If they crash suddenly after a drug, treat as anaphylaxis — not as hypotension.”
5️⃣ Local Anesthetic Systemic Toxicity (LAST)
— When the Drug That Numbs Suddenly Threatens Life
💉 What Is LAST?
Local Anesthetic Systemic Toxicity (LAST) is a potentially fatal reaction caused by excessive plasma levels of local anesthetics — due to:
- Intravascular injection
- Overdose (especially in small or lean patients)
- Rapid absorption from vascular areas (e.g., intercostals, scalp)
🧠 When to Suspect LAST
| Phase | Signs & Symptoms |
|---|---|
| CNS excitation | Agitation, tinnitus, circumoral numbness, metallic taste, seizures |
| CNS depression | Drowsiness, coma, respiratory arrest |
| Cardiac toxicity | Bradycardia, widened QRS, VT/VF, asystole |
⚠️ Many cases occur within 1–5 minutes of injection, especially if not aspirated properly before injecting.
🔬 Which Agents Are More Dangerous?
| High Risk | Lower Risk |
|---|---|
| Bupivacaine | Lidocaine (moderate) |
| Ropivacaine (less) | Chloroprocaine (rapid metabolism) |
Bupivacaine is highly cardiotoxic — binds myocardial Na⁺ channels firmly.
🔍 Differential Diagnosis to Rule Out
- Seizure due to hypoglycemia
- Anaphylaxis (if hypotension + rash)
- Vasovagal syncope
- Hypoxia or hypercarbia under sedation
⚡ Immediate Management of LAST
✅ Stepwise Protocol
1️⃣ Stop Local Anesthetic Injection Immediately
— Announce: “SUSPECTED LAST!”
2️⃣ Call for Help + 100% Oxygen
— Avoid hypoxia/acidosis (they potentiate toxicity)
— Secure airway — intubate early if needed
3️⃣ Manage Seizures
| Drug | Dose | Note |
|---|---|---|
| Midazolam | 1–2 mg IV | First-line, rapid acting |
| Diazepam | 5–10 mg IV | Longer onset |
| Propofol | 1 mg/kg IV | If no hypotension |
| 🛑 Avoid | Large propofol doses in CV collapse | Can worsen hypotension |
4️⃣ Administer Lipid Emulsion Therapy
This is the antidote — do not delay!
| Lipid 20% | Dose |
|---|---|
| Initial bolus | 1.5 mL/kg IV over 1 min |
| Continuous infusion | 0.25 mL/kg/min IV (for 30–60 min) |
| Repeat bolus | Once or twice for persistent CV instability |
| Max dose | 10 mL/kg over first 30 min |
🧠 Lipid “soaks up” free anesthetic molecules — like a sponge.
5️⃣ Treat Cardiac Arrest According to ACLS, with Modifications
| Standard ACLS | Modified for LAST |
|---|---|
| Epinephrine 1 mg IV | Use lower doses (10–100 mcg) |
| Amiodarone, CPR, defib | ✅ Continue as per protocol |
| Avoid: lidocaine, vasopressin | Can worsen toxicity |
🛠️ Low-Resource Setting Tips
-
No lipid emulsion?
🔴 There is no full substitute — but provide O₂, seizure control, airway, and transport
🧠 If only Intralipid available, still use it cautiously — better than none. -
No midazolam? Use low-dose propofol or IV diazepam
-
Store Lipid Emulsion 20% wherever regional anesthesia is practiced
📦 Prevention is Better Than Crisis
| Strategy | Why |
|---|---|
| Always aspirate before injecting | Detects intravascular placement |
| Use ultrasound guidance | Increases safety in regional blocks |
| Use lowest effective dose | Especially in elderly, frail, or low BMI |
| Monitor continuously | ECG, SpO₂, ETCO₂ during blocks |
| Have lipid rescue kit nearby | Label and train staff on its use |
💡 Clinical Pearl
“The difference between numbing a nerve and stopping a heart is just 1 mL in the wrong place.
But 1.5 mL/kg of lipid can bring the heart back.”
🧪 ⚠️ Bonus Box: Methemoglobinemia — When Blood Can’t Carry Oxygen
❓ What Is It?
Methemoglobinemia occurs when iron in hemoglobin is oxidized from Fe²⁺ to Fe³⁺, preventing it from binding and releasing oxygen.
🧠 Even with normal lungs and oxygen supply, tissues become hypoxic.
💉 Common Triggers in Anesthesia
| Agent | Notes |
|---|---|
| Lidocaine | Especially high-dose IV or topical use |
| Prilocaine | Known dose-dependent risk >6 mg/kg |
| Benzocaine sprays | Common in upper airway endoscopy, awake intubation |
| Nitroglycerin, Nitroprusside | Also oxidizing drugs |
🧠 When to Suspect
- Patient becomes cyanotic, but SpO₂ stays around 85% and doesn't respond to 100% O₂
- Chocolate-brown blood in syringe or suction
- Low PaO₂–SpO₂ correlation on ABG (PaO₂ normal, SpO₂ low)
- Tachycardia, confusion, lethargy if severe
🧪 Confirm the Diagnosis
- Co-oximetry (on blood gas) shows MetHb >1–2%
→ Symptoms usually start >10–15%
→ Life-threatening >30–40%
💊 Treatment
| Drug | Dose | Note |
|---|---|---|
| Methylene blue | 1–2 mg/kg IV over 5 min | Repeat once if needed (max 7 mg/kg) |
| Vitamin C (ascorbic acid) | 1–2 g IV (if MB unavailable) | Slower, less effective |
| O₂ therapy | 100% O₂ to support tissue oxygenation | Adjunct only |
🛠️ Low-Resource Pearls
- No methylene blue? Use high-dose vitamin C + O₂
- Recognize “saturation gap” — SpO₂ 85%, PaO₂ normal
- Avoid using benzocaine sprays in awake intubation when unmonitored
💡 Clinical Pearl
“If the blood is brown and the monitor won’t climb, it’s not your ventilator — it’s your hemoglobin.”
6️⃣ Malignant Hyperthermia (MH)
— The Hidden Fire Behind the Anesthesia Curtain
❗ What Is Malignant Hyperthermia?
MH is a rare, inherited hypermetabolic crisis of skeletal muscle triggered by:
- Volatile anesthetics (e.g., sevoflurane, halothane, isoflurane)
- Depolarizing muscle relaxants (especially suxamethonium)
In genetically susceptible individuals (mutation in RYR1 gene), these agents cause uncontrolled calcium release, leading to:
- Sustained muscle contraction
- Heat generation
- Metabolic acidosis
- Death if untreated
⚠️ When to Suspect
Often develops within 30 min of induction but may be delayed up to 12 hours.
🧠 Classic Signs — Mnemonic: "HOT STIFF ACID"
| Letter | Clue |
|---|---|
| H | Hyperthermia (late sign, rapid ↑ >1°C every 5 min) |
| O | O₂ consumption ↑ — desaturation, ↑ ETCO₂ |
| T | Tachycardia — sudden, unexplained |
| S | Stiff muscles — rigid jaw (masseter spasm), generalized rigidity |
| T | Tachypnea / ↑ minute ventilation (in spontaneous breathing) |
| I | Instability — hemodynamic, arrhythmias |
| F | Fever (late and dramatic) |
| A | Acidosis (metabolic + respiratory) |
| C | Capnography — ↑↑ ETCO₂ despite ventilation |
| I | Increased K⁺, CK, myoglobin |
| D | Dark urine (myoglobinuria → renal failure risk) |
💡 Red Flag Early Signs
- Sudden ↑ in ETCO₂ (>55 mmHg) with normal ventilation
- Masseter spasm after suxamethonium
- Unexplained sinus tachycardia + rigidity
🧠 Don’t wait for fever — hyperthermia is a late sign.
🚨 Management — Treat Fast, Don’t Confirm First
✅ Step-by-Step Emergency Management
🔸 1. Discontinue All Triggers Immediately
- Stop volatile agent
- Stop suxamethonium
- Switch to 100% O₂, increase fresh gas flow
🔸 2. Call for Help + Announce "Suspected MH"
- Inform surgical team
- Prepare Dantrolene ASAP
🔸 3. Administer Dantrolene
| Drug | Initial Dose | Repeat Dosing |
|---|---|---|
| Dantrolene | 2.5 mg/kg IV (ASAP) | Repeat q5–10 min until stable (max ~10 mg/kg) |
| Ryanodex® | More concentrated; same dose | Easier preparation (1 vial = 250 mg) |
💉 Continue dantrolene for 24–48 hrs post-crisis to prevent recrudescence
💊 Supportive Treatment
| Issue | Intervention |
|---|---|
| Hyperkalemia | Calcium gluconate, insulin + glucose, furosemide |
| Acidosis | Sodium bicarbonate (if pH <7.2) |
| Arrhythmias | Avoid calcium channel blockers with dantrolene! |
| Hyperthermia | Active cooling: IV saline, ice packs, lavage |
| Renal protection | Fluids, mannitol, furosemide — monitor urine output |
🎯 Target urine output: >2 mL/kg/hr to flush myoglobin
🛠️ MH Protocol in Low-Resource Settings
-
No dantrolene?
- Use supportive care only
- Cool aggressively, treat hyperkalemia and acidosis
- Transfer immediately to nearest center with MH supplies
-
No ETCO₂ monitor?
- Look for rigidity + sudden tachycardia + unexplained desaturation
- Use core temperature monitoring if available
-
Use safe agents in MH-susceptible patients:
✅ Propofol, opioids, non-depolarizing relaxants (rocuronium)
❌ Avoid sevoflurane, halothane, suxamethonium
📦 MH Cart Essentials
- Dantrolene vials (or Ryanodex)
- Sodium bicarbonate
- Ice packs, cooling fluids
- Furosemide, mannitol
- Sterile syringes, mixing saline
- MH protocol sheet on wall
🧬 After the Crisis:
- Send CK, renal panel, ABG, coagulation
- Refer for genetic testing (RYR1 mutation)
- MH hotline if available
- Document in the chart and warn family
→ This is heritable (autosomal dominant)
💡 Clinical Pearl
“If they’re getting stiffer, hotter, and more acidic…
Don’t wait — dantrolene saves lives, not diagnosis.”
7️⃣ Major Hemorrhage & Coagulopathy in the OR
— When Bleeding Becomes the Battle
🩸 Why It’s Critical
Uncontrolled intraoperative bleeding can lead to:
- Hypovolemic shock
- Coagulopathy
- Hypothermia
- Acidosis
- → The deadly triad that spirals into death without mercy
Early recognition and structured response save lives — especially in trauma, OB, liver resection, and vascular surgery.
⚠️ When to Suspect Major Bleed
| Clue | Interpretation |
|---|---|
| Sudden ↓ in BP + ↑ HR | Hypovolemia or hidden bleed |
| Soaked sponges, suction >500 mL | Active hemorrhage |
| Darkening field, surgeon struggling | Bleeding deep in cavity |
| ↓ SpO₂, ↑ lactate, ↓ urine | Hypoperfusion signs |
| ↓ ETCO₂ (if shock develops) | Poor perfusion |
🔍 Causes of Coagulopathy Intraop
- Dilutional (massive transfusion)
- Consumptive (DIC, sepsis, trauma)
- Liver failure / uremia
- Anticoagulants (warfarin, DOACs, heparin)
- Hypothermia (<35°C impairs platelet function)
⚡ Stepwise Management
🔸 1. Resuscitate & Replace Volume
| Fluid | Role |
|---|---|
| Crystalloids | Initial bolus (1–2 L) |
| Blood products | Replace oxygen-carrying capacity |
| Colloids | Use with caution (can impair clotting) |
🧠 Don't delay blood if major loss is suspected
🔸 2. Activate Massive Transfusion Protocol (MTP)
1:1:1 ratio of:
- PRBCs (packed RBCs)
- FFP (fresh frozen plasma)
- Platelets
Start when:
-
1500 mL lost within 10–15 min
-
50% blood volume lost within 3 hrs
- Ongoing bleeding + shock signs
🔸 3. Warm the Patient!
- Use fluid warmers, blankets, warm ambient OR
- Hypothermia worsens coagulopathy
🔸 4. Correct Coagulopathy
| Product / Drug | Indication |
|---|---|
| FFP (15–20 mL/kg) | Prolonged INR, bleeding |
| Platelets | Plt <50,000 with bleeding |
| Cryoprecipitate | Fibrinogen <1.5 g/L |
| Tranexamic acid (TXA) | Trauma, OB hemorrhage (1 g over 10 min + 1 g over 8 hrs) |
| Prothrombin Complex Concentrate (PCC) | Reversal of warfarin or DOACs |
| Calcium gluconate | 10 mL of 10% IV every 4 units blood (prevent citrate toxicity) |
🔸 5. Use Point-of-Care Tests (If Available)
| Test | What It Shows |
|---|---|
| TEG / ROTEM | Clot strength, fibrinogen, platelets, fibrinolysis |
| ABG + Lactate | Perfusion, acidosis, hypoxia |
| ACT / aPTT / INR | Coagulation status |
🛠️ Low-Resource Setting Adaptations
- No FFP? Use fresh whole blood if available
- No platelets? Consider DDAVP (0.3 mcg/kg IV) to boost platelet function
- No TXA IV? Use oral tablets crushed + NG tube or rectal
- Monitor clinically: BP, urine, sponge weight, surgical feedback
📉 Clinical Case Example
A 42-year-old woman undergoing emergency hysterectomy begins to ooze from IV sites, BP drops to 70/40, HR 130.
Suction canister shows 1.2 L blood. Temp is 34°C. INR returns at 2.4.
Diagnosis: Major hemorrhage with early DIC.
Action: Warm patient, give TXA, initiate MTP (PRBC + FFP + platelets), send TEG, give cryo.
💡 Clinical Pearl
“The clock starts when the bleeding starts — not when the blood arrives.”
Think ahead. Move fast. Stay structured.
8️⃣ Hypoxia & Hypercapnia in the OR
— When Oxygen Fades and Carbon Dioxide Rises
🧠 Why This Section Matters
While anesthetized, patients don’t complain of shortness of breath.
So when SpO₂ drops or ETCO₂ rises, we must:
- Interpret data rapidly
- Distinguish machine issues from patient deterioration
- Act before arrest, brain injury, or acidosis sets in
🔍 1. Hypoxia (Desaturation)
⚠️ When to Suspect
| Sign | Clue |
|---|---|
| ↓ SpO₂ < 90% | Poor oxygenation |
| ↓ ETCO₂ (if apnea or arrest) | Indicates low ventilation or perfusion |
| ↑ HR → Bradycardia | Early then late hypoxic sign in children |
| Cyanosis (late) | Often masked by lighting, anemia |
🔎 Stepwise Differential Diagnosis — Mnemonic: "DOPE + 3 P’s"
| Cause | Example |
|---|---|
| Displacement | ETT dislodged or right mainstem |
| Obstruction | Mucus plug, kinking, secretions, bronchospasm |
| Pneumothorax | Tension → sudden hypoxia + ↑ PIP + hypotension |
| Equipment failure | Circuit disconnection, O₂ failure |
| Pulmonary embolism | Sudden ↓ ETCO₂, ↑ HR, ↓ BP |
| Position-related | Lateral decubitus or laparoscopic compression |
| Pulmonary edema | Pink frothy sputum, crackles, ↓ compliance |
✅ Stepwise Response to Hypoxia
- Call for help
- 100% O₂ — bag manually if in doubt
- Check ETT position & cuff
- Suction airway
- Check for bronchospasm or obstruction
- Auscultate both lungs — equal? absent?
- Switch to self-inflating bag if ventilator suspect
- Rule out tension pneumothorax (needle if needed)
🔄 Expanded Diagnostic Sidebar:
1- Pulmonary Embolism
🚨 Can Pulmonary Embolism (PE) Happen Intra- or Postoperatively?
✅ Yes, absolutely.
⏱️ Timing:
- Intraoperative PE → rare but catastrophic, often in patients with:
- DVT + surgical manipulation (esp. orthopedic, pelvic)
- Hypercoagulable states (e.g., malignancy, pregnancy, trauma)
- Postoperative PE → within 48–72 hrs most common
- Orthopedic, pelvic, spinal, long surgeries
- No prophylaxis or delayed mobilization
🧠 How to Recognize PE Intraoperatively
| Sign | Clue |
|---|---|
| Sudden ↓ in SpO₂ | Often unexplained |
| Sudden ↓ ETCO₂ | From ↓ perfusion (dead space) |
| ↑ HR, ↓ BP | Shocky, unexplained tachycardia |
| ↓ end-tidal + rising PaCO₂ | Widening gradient |
| ECG: Sinus tachy, S1Q3T3 | Classic but rare |
| CVP ↑ | If monitored, suggests RV strain |
🧪 Suspect in:
- Unexplained desaturation + hypotension
- Sudden drop in ETCO₂ with no airway issue
- History of DVT or recent trauma/pelvic procedure
🧑⚕️ Immediate Management of Suspected PE
| Action | Why |
|---|---|
| 100% O₂ | Maximize oxygenation |
| Call for help | Anesthesia + surgical team |
| Support BP | Noradrenaline / phenylephrine IV |
| Consider Heparin (postop) | If confirmed or strongly suspected |
| Echo if available | RV dilatation, D-shaped LV = PE |
| CT-PA / V/Q scan | After stabilizing (postop or ICU) |
🧠 Intraop cardiac arrest → start CPR, consider thrombolysis only if diagnosis is clear and patient is unresuscitable.
I- Pulmonary Edema
💦 Pulmonary Edema (Cardiogenic or Volume Overload)
| Cause | Signs |
|---|---|
| LV failure | Crackles, ↑ CVP, CXR: Bat-wing edema |
| Fluid overload | High CVP, ↑ weight, low Na⁺ |
| Renal failure | No urine output, anasarca |
💊 Management of Pulmonary Edema (Cardiogenic or Fluid Overload)
| Action | Purpose |
|---|---|
| Position upright | Improves ventilation-perfusion matching |
| High-flow O₂ / CPAP / BiPAP | Decreases preload and improves oxygenation |
| IV furosemide 20–40 mg | Diuresis — monitor urine output |
| Morphine (2–4 mg IV) optional | Decreases anxiety, preload (controversial) |
| IV nitroglycerin | Reduces preload and afterload |
| Inotropes (dobutamine) | If LV failure with hypotension |
| Restrict fluids | Prevent ongoing overload |
🧠 Target BP support + oxygenation + fluid offloading
🛠️ Low-Resource Adaptations:
- No CPAP? Use manual PEEP valve or high-flow O₂ with face mask
- No furosemide IV? Use oral furosemide + O₂ + upright positioning
- Monitor urine output with foley; even visual estimation matters
💡 Clinical Pearl:
“If crackles rise and the lungs drown, don’t reach for bronchodilators — reach for diuretics and PEEP.”
II- Fat Embolism Syndrome (FES)
— The Hidden Threat After Bone Fractures
🧠 What Is It?
Fat Embolism Syndrome (FES) occurs when fat droplets from marrow or soft tissue enter the bloodstream and obstruct capillaries — especially in the lungs, brain, and skin.
Often seen after:
- Long bone fractures (femur, tibia)
- Pelvic fractures
- Orthopedic trauma surgery
- Burns or massive soft tissue injury
⏱️ Onset
- Usually 12–72 hours post-injury or surgery
- May occur intraoperatively, particularly during reaming of bone
⚠️ Classic Triad
| Sign | Clinical Clue |
|---|---|
| Hypoxia | ↓ SpO₂, ↑ RR, ↓ PaO₂ |
| Neurologic changes | Confusion, agitation, seizures, coma |
| Petechial rash | Axilla, conjunctiva, chest (in <50%) |
Often accompanied by:
- Fever
- Tachycardia
- Drop in ETCO₂ intraop
🧪 Investigations (if suspected)
| Test | Findings |
|---|---|
| ABG | Hypoxemia, ↑ A–a gradient |
| Chest X-ray | Bilateral infiltrates, “snowstorm” appearance |
| CBC | Anemia, thrombocytopenia |
| Coagulation | Mildly deranged, but not full DIC |
🩺 Management
No antidote — supportive care is key
| Strategy | Why |
|---|---|
| High-flow O₂ / Intubation | Correct hypoxemia |
| Protect airway | Sedation if agitated |
| Fluids | Maintain perfusion |
| Steroids | Controversial; some studies show benefit |
| DVT prophylaxis | LMWH or heparin to prevent true PE |
🛠️ Tips for Low-Resource Settings
- No ABG? Rely on SpO₂, RR, mental status
- No CT? Use clinical triad + CXR
- Suspect in young trauma patients who deteriorate without bleeding
🧠 Clinical Pearl
“If your femur breaks and your mind follows 24 hours later — suspect fat embolism.
Especially if oxygen falls and rash rises.”
🔥 2. Hypercapnia (↑ ETCO₂)
🧠 What Is It?
| Normal ETCO₂ = 35–45 mmHg
High ETCO₂ can indicate:
- ↓ ventilation
- ↑ CO₂ production
- Rebreathing
⚠️ Causes of Hypercapnia
| Category | Examples |
|---|---|
| ↓ Minute ventilation | Inadequate tidal volume or RR |
| Rebreathing | Exhausted soda lime, stuck valve |
| ↑ Metabolism | MH, thyrotoxicosis, fever, seizures |
| CO₂ insufflation | During laparoscopy |
| Obstruction | Bronchospasm, kinked tube |
✅ Stepwise Management of Hypercapnia
- Confirm waveform & number
- Check RR and tidal volume
- Switch to manual bag ventilation
- Suction for obstruction
- Increase minute ventilation (RR and/or Vt)
- Treat underlying cause (MH, circuit issue, rebreathing)
📈 Capnography Patterns:
| Waveform | Interpretation |
|---|---|
| Flat or absent | Disconnection, apnea, arrest |
| Shark fin (sloped) | Bronchospasm |
| Gradual rise | Hypoventilation |
| Sudden drop | Pulmonary embolism or disconnection |
🧠 ETCO₂ is your real-time window to ventilation & perfusion.
🛠️ Low-Resource Tips
- No capnograph? Watch bag movement, chest rise, SpO₂ trends
- No oxygen analyzer? Check color of reservoir bag and patient’s color
- No ABG? Use capillary or venous blood gas for CO₂ estimate
- Still desaturating? Consider changing circuit or using ambu bag + oxygen
💡 Clinical Pearl
“Desaturation is a symptom. Capnography is your stethoscope.
Use it to diagnose — not just display.”
🧱 Cement Embolism (Bone Cement Implantation Syndrome — BCIS)
— The Invisible Killer of Hip Cementing Procedures
🧠 What Is It?
Bone Cement Implantation Syndrome (BCIS) is a rare but life-threatening complication of cemented prosthetic surgery — especially hip arthroplasty.
Acrylic bone cement releases monomer gases and fat droplets, which may enter the venous system under pressure and embolize to the lungs, causing:
- Right ventricular failure
- Pulmonary hypertension
- Cardiovascular collapse
⏱️ When Does It Happen?
| Timing | Trigger |
|---|---|
| During cement insertion | Especially in femoral canal |
| Prosthesis insertion | Causes pressure surge → embolization |
| Joint reduction or limb manipulation | Dislodges embolic material into circulation |
⚠️ How to Recognize Intraoperatively
| Sign | Clue |
|---|---|
| Sudden ↓ in ETCO₂ | Suggests ↓ pulmonary perfusion |
| Sudden ↓ in SpO₂ | Hypoxia without clear airway cause |
| Hypotension + Bradycardia | Due to RV failure |
| Cardiac arrest | Often pulseless electrical activity (PEA) |
| CVP ↑ (if monitored) | Indicates RV strain |
🧬 Why It Happens
- Increased intramedullary pressure
- Microfractures in venous sinusoids
- Entry of cement particles, fat, air, and marrow into bloodstream
- Triggers pulmonary vascular spasm, PE-like picture, and RV overload
💉 Immediate Management
| Step | Goal |
|---|---|
| 100% O₂ | Oxygenate tissues |
| Trendelenburg position | Improve RV preload |
| Vasopressors (noradrenaline, phenylephrine) | Support RV function |
| CPR if needed | Follow ACLS — high suspicion for PE-type cause |
| Avoid excessive fluids | RV can’t handle overload |
🛠️ Low-Resource Settings Tips
- No ETCO₂ monitor? Look for sudden cyanosis, pulse loss, chest asystole
- No echo? Watch BP + HR + loss of waveforms closely
- Prevention: Use uncemented prosthesis or venting techniques when possible
🧯 Prevention in the OR
| Technique | Why |
|---|---|
| Use high-flow O₂ before cementing | Oxygen reserve |
| Avoid deep sedation | Keep patient responsive (in spinal) |
| Communicate with surgeon | “Cement going in” warning to prepare |
| Use un-cemented prosthesis in high-risk patients | Reduce risk |
💡 Clinical Pearl
“If the hip is cemented and the heart suddenly quits — don’t look at the airway. Look at the cement.”
9️⃣ Equipment & Circuit Failures
🔌 When It's Not the Patient — It's the Machine
🧠 Why It Matters
Perioperative emergencies can often mimic physiologic collapse — but the true culprit may be mechanical. Misdiagnosis can lead to unnecessary CPR, drug overdose, or delayed response.
“If SpO₂ drops, ETCO₂ disappears, and the BP tanks — check the machine before you shock the patient.”
🔎 Common Equipment Failures
| Failure | Clue | Danger |
|---|---|---|
| 🔌 Oxygen supply failure | Low pipeline pressure, empty backup cylinder | Hypoxia, circuit collapse |
| 💨 Ventilator malfunction | Bellows not filling, alarm sounds, no chest movement | Apnea, hypercapnia, hypoxia |
| 🌫️ Soda lime exhausted | Rising inspired CO₂, hypercapnia, tachycardia | CO₂ rebreathing |
| 🚫 Circuit disconnection | Sudden drop in ETCO₂ + SpO₂, no breath sounds | Apnea, unnoticed for minutes |
| 🧱 Filter or HME blockage | High airway pressures, wheeze-like sound, SpO₂ ↓ | High PIP, barotrauma, false asthma |
| ⚠️ Misassembled circuit | Tight bag, high resistance, no ventilation | Immediate danger if unnoticed |
| 🔃 Ventilator valve stuck | No expiratory flow, rising pressure | Air trapping, barotrauma |
🛠️ Troubleshooting Flowchart
🧾 Symptoms:
- Sudden desaturation (SpO₂ ↓)
- Flat ETCO₂
- No chest rise
- High airway pressure
- Alarms from ventilator
➡️ Action Steps:
- CALL FOR HELP — Always initiate teamwork early
- Switch to manual bagging
▫️ Check compliance — stiff or floppy lungs?
▫️ Observe chest movement - Check circuit integrity
▫️ Connections tight? Any kinks?
▫️ Is HME/filter clogged? - Confirm oxygen supply
▫️ Backup cylinder open? Pipeline connected? - Listen to the patient
▫️ If bag is compliant & patient improves → machine problem
▫️ If still no ventilation → patient or ETT problem - Consider replacing the entire circuit if in doubt
🧪 What to Look For on Monitors
| Parameter | Machine Issue Clues |
|---|---|
| ETCO₂ ↓ or flat | Disconnection, apnea, circuit block |
| SpO₂ ↓ | O₂ supply, circuit failure, real disease |
| PIP ↑ | Kinked ETT, blocked filter, bronchospasm |
| Volumes ↓ | Leak, disconnect, ventilator failure |
🧯 Emergency Rescue Measures
| Situation | Rescue Strategy |
|---|---|
| Total ventilator failure | Switch to self-inflating bag + 100% O₂ |
| Soda lime exhaustion | Bypass canister if no spare, increase flow |
| Oxygen supply collapse | Open cylinder O₂, switch to ambu bag |
| No monitor functioning | Use stethoscope, pulse, skin signs |
🧰 Tips for Low-Resource Settings
- Always have a self-inflating ambu bag in the room
- Colorimetric CO₂ detector if no waveform capnograph
- Train staff to assemble and test circuits pre-op
- Spare filter, circuit, and O₂ key nearby always
- In power cuts — use manual bagging with room air if no O₂
💡 Clinical Pearl
“Don’t paralyze your patient until you’ve paralyzed your doubts about your machine.”
🔟 Pediatric-Specific Emergencies
🧸 Small Bodies, Big Crises – Pediatric OR & ICU
🧠 Why It's Different
Pediatric patients are not mini adults.
Their physiology is faster, their reserves are smaller, and their margin for error is razor-thin.
“In a child, hypoxia doesn’t knock — it crashes the door.”
1️⃣ Bradycardia = Hypoxia Until Proven Otherwise
▪️ Most pediatric bradycardia is due to hypoxia, not intrinsic conduction problems.
▪️ Immediate ventilation and oxygenation take priority — not atropine first.
| Sign | Clue |
|---|---|
| HR < 60 + weak pulse | Likely hypoxic bradycardia |
| ETCO₂ ↓ + SpO₂ ↓ | Ventilatory failure |
| High vagal tone | Possible if intubation, suction, or rectal stimulus (e.g., anal stretch) |
🔹 Management
- 100% O₂, manual ventilation
- Chest compressions if HR < 60
- Atropine 0.02 mg/kg if vagal cause suspected
- Epinephrine IV/IO 0.01 mg/kg
2️⃣ Post-Extubation Stridor & Airway Obstruction
▪️ Common in young children, especially after repeated attempts or prolonged intubation.
▪️ Often due to laryngeal edema or subglottic narrowing.
| Clue | Suggestion |
|---|---|
| Inspiratory stridor + retractions | Laryngeal edema likely |
| Hoarseness, barking cough | Croup-style presentation |
🔹 Management
- Racemic epinephrine nebulizer
- Dexamethasone IV 0.6 mg/kg
- Reintubate if worsening or desaturation
3️⃣ Airway Crisis: Small Tube, Big Risk
▪️ Minor tube dislodgment = major ventilation failure
▪️ Capnography, breath sounds, and chest rise are your compass
▪️ Always have a smaller tube ready for reintubation
4️⃣ Drug Dose Miscalculation
▪️ Pediatric drug errors are catastrophic
▪️ Always double-check doses by weight
▪️ Use Broselow tape, apps, or printed charts
📋 Emergency Drug Dosing — Pediatric Quick Reference
(IV/IO unless otherwise stated)
🔹 Epinephrine (1:10,000): 0.01 mg/kg
🔹 Atropine: 0.02 mg/kg (minimum 0.1 mg, max 0.5 mg per dose)
🔹 Midazolam: 0.05–0.1 mg/kg
🔹 Ketamine: 1–2 mg/kg IV | 4–5 mg/kg IM
🔹 Suxamethonium: 1–2 mg/kg
🔹 Rocuronium: 0.6–1.2 mg/kg
🔹 Fentanyl: 1–2 mcg/kg
🔹 Morphine: 0.05–0.1 mg/kg
🔹 Dextrose 10%: 2 mL/kg bolus
🔹 Calcium Gluconate 10%: 0.5–1 mL/kg (slowly over 10 min)
🔹 Lidocaine (antiarrhythmic): 1 mg/kg
🔹 Adenosine: 0.1 mg/kg (1st dose), 0.2 mg/kg (2nd dose)
🔹 Naloxone: 0.01 mg/kg (repeat q2–3 min if needed)
🔹 Amiodarone: 5 mg/kg over 20–60 min
🔹 Magnesium Sulfate: 25–50 mg/kg (max 2 grams)
🔹 Dexamethasone: 0.6 mg/kg (max 10 mg)5️⃣ Hypoglycemia Under Anesthesia
▪️ Infants and neonates have limited glycogen stores
▪️ Monitor glucose intraop in prolonged or emergency surgeries
🔹 Treat with
- Dextrose 10% IV at 2 mL/kg bolus
- Then D5 or D10 maintenance infusion
6️⃣ IV Access Challenges
▪️ IO access is life-saving when IV fails
▪️ Use tibial IO if < 6 years and arrest or shock
🔹 Landmark:
1–2 cm below tibial tuberosity, medial surface
7️⃣ Temperature Instability
▪️ Hypothermia causes bradycardia, coagulation impairment
▪️ Prewarm the OR, use warmed fluids, forced air warmers
💡 Clinical Pearl
“A quiet child on the OR table isn’t always stable — it could be the calm before hypoxia. Watch, listen, act early.”
1️⃣1️⃣ Hypertensive Spikes & Crises
🩸 “Pressure is rising — is it pain, panic, or pathology?”
🧠 Why This Matters
Hypertension during anesthesia isn’t always benign.
Sudden SBP >180 mmHg or DBP >120 mmHg, especially in a patient with cardiovascular disease, may precipitate:
- Stroke (especially in elderly with fragile vessels)
- MI (due to increased myocardial oxygen demand)
- Aortic dissection (in high-risk individuals)
- Bleeding (in neuro, ENT, eye, or spine surgeries)
⚠️ Common Intraoperative Triggers
| Cause | Clue |
|---|---|
| Light anesthesia | Sudden ↑ BP/HR when stimulation starts |
| Full bladder or surgical pain | ↑ BP despite deep sedation |
| Hypoxia, hypercarbia | Gradual ↑ BP + ↑ HR |
| Pre-existing HTN (undocumented) | Consistently high BP despite good anesthesia |
| Drug error (e.g. phenylephrine bolus) | Sharp spike in BP, reflex bradycardia |
| Intubation/extubation response | Sudden ↑ BP/HR — typical sympathetic surge |
🔍 How to Recognize
| Monitor Clue | Interpretation |
|---|---|
| ↑ BP + ↑ HR | Likely pain, light plane, or anxiety |
| ↑ BP + ↓ HR | Possible autonomic reflex (e.g., drug-induced) |
| ↑ BP + ST changes | Suspect ischemia or increased cardiac workload |
🧑⚕️ Immediate Management Strategy
🔹 Stepwise Response
-
Deepen anesthesia
- Increase volatile agent (e.g., sevoflurane)
- Give propofol bolus (0.5–1 mg/kg)
-
Treat pain
- Fentanyl bolus (1 mcg/kg)
- Consider paracetamol IV or regional block
-
Control BP directly if needed
- Labetalol IV 5–10 mg over 2 mins
- Esmolol IV 0.5 mg/kg (or infusion)
- Hydralazine 5–10 mg IV (esp. in pregnancy)
- Nitroglycerin/Nicardipine infusion if persistent
-
Investigate & rule out serious causes
- ECG (ischemia?)
- ABG (hypoxia/hypercarbia?)
- Full review of recent drugs given
💡 Special Case: Postoperative HTN
- Common during emergence, recovery, or PACU stay
- May be due to pain, bladder distention, agitation, or residual sympathetic tone
- Control with small titrated doses:
- Labetalol 5–10 mg IV
- Clonidine 1 mcg/kg IV slowly
- Restart home antihypertensives if possible
🌍 Tips in Low-Resource Settings
- If no IV labetalol → use IV hydralazine slowly
- Oral nifedipine (bite-and-swallow) still used but can cause rebound — caution!
- IM diazepam may help if anxiety is severe
🧠 Clinical Pearl
“Not every spike is a stroke — but every spike must earn your respect.”
1️⃣2️⃣ Low-Resource Toolbox
🧰 “What if you had to save a life — with nothing but your brain, your hands, and your heart?”
🧨 No Dantrolene — Suspected Malignant Hyperthermia (MH)
In remote ORs without dantrolene:
- Stop all volatile agents + suxamethonium immediately
- Hyperventilate with 100% O₂
- Initiate external cooling:
- Ice packs to groin, axilla, neck
- Cold IV fluids if possible
- Treat symptoms:
- Tachycardia + arrhythmia → beta blockers (if stable)
- Acidosis → sodium bicarbonate
- Hyperkalemia → insulin + dextrose + salbutamol
📌 If available, use propranolol or esmolol to control HR, but monitor BP.
🧠 Pearl: Even without dantrolene, rapid cooling + O₂ + vigilance can delay catastrophe until transfer.
💉 No Lipid Rescue — LAST (Local Anesthetic Systemic Toxicity)
If lipid emulsion unavailable in a LAST scenario:
- Stop injection immediately
- Call for help, initiate advanced cardiac life support (ACLS)
- Support airway + ventilation with 100% O₂
- Seizure control:
- Use midazolam, propofol, or thiopental if available
- Avoid vasopressin, calcium channel blockers, beta-blockers
- If cardiac arrest:
- Use low-dose adrenaline (≤1 mcg/kg)
- Continue CPR, oxygen, and manual ventilation
🧠 Pearl: Do not abandon the patient — lipid is ideal, but airway and oxygen still save lives.
📉 No Capnography — Ventilation Monitoring Hacks
Without EtCO₂, rely on:
- Chest rise & RR
- SpO₂ trends
- Auscultation for bilateral air entry
- Manual reservoir bag feedback (tight = bronchospasm, loose = leak)
- ABG if available after 10–15 mins post-intubation
🛠️ In peds, watch for:
- Nasal flaring
- Chest wall retraction
- Cyanosis despite chest rise = poor alveolar ventilation
💨 Manual Airway & Rescue Ventilation
No ventilator?
- AMBU bag with PEEP valve
- Ensure tight mask seal, 2-hand technique
- If ETT dislodged → oral airway + mask until re-intubation
- No airway? Use:
- NPA or OPA
- 14G needle cricothyrotomy (landmark: thyroid cartilage → 1 cm below)
🧠 “The best ventilator is your hand when your mind is calm.”
💊 Crash Cart Essentials — The Emergency Ten
If your OR or ER has only 10 meds, keep:
- Adrenaline (Epinephrine) — shock, arrest, anaphylaxis
- Atropine — bradycardia, asystole
- Ketamine — induction, sedation, shock
- Midazolam — seizures, agitation, premed
- Propofol — induction, control ICP, status epilepticus
- Rocuronium or Sux — paralysis
- Fentanyl — analgesia
- Dextrose 10% — hypoglycemia, pediatric resus
- Hydrocortisone — shock, allergy, adrenal support
- Salbutamol — bronchospasm, hyperkalemia
✅ Bonus: Normal saline and O₂ — the forgotten essentials.
🧠 Clinical Pearl:
“In Baghdad, in Kut, in Wainiki — we’ve saved lives with nothing but will and wisdom.
This section honors that strength.”
1️⃣3️⃣ Emergency Drug Table — Adult & Pediatric Dosing
| Drug | Indication | Adult Dose | Pediatric Dose |
|---|---|---|---|
| Adrenaline (Epinephrine) | Cardiac arrest, anaphylaxis | 1 mg IV every 3–5 min (1:10,000) 0.3–0.5 mg IM (1:1,000) |
10 mcg/kg IV (max 1 mg) 0.01 mg/kg IM (max 0.3 mg) |
| Atropine | Bradycardia, asystole | 0.5–1 mg IV, repeat q3–5 min (max 3 mg) | 0.02 mg/kg IV (min 0.1 mg, max 0.5 mg child / 1 mg adolescent) |
| Amiodarone | Refractory VF/pVT | 300 mg IV bolus, then 150 mg if needed | 5 mg/kg IV over 20–60 min (max 300 mg) |
| Adenosine | Supraventricular tachycardia (SVT) | 6 mg rapid IV push, may repeat with 12 mg | 0.1 mg/kg IV push → 0.2 mg/kg if no response (max 12 mg) |
| Lidocaine | VT/VF, alternative to amiodarone | 1–1.5 mg/kg IV bolus; max 3 mg/kg | 1 mg/kg IV bolus (max 100 mg) |
| Magnesium sulfate | Torsades de pointes, severe asthma | 1–2 g IV over 10–20 min | 25–50 mg/kg IV over 10–20 min (max 2 g) |
| Dextrose 10% | Hypoglycemia | 100–200 ml IV | 2–5 ml/kg IV |
| Calcium gluconate | Hyperkalemia, hypocalcemia | 1 g IV slowly over 10 min | 60–100 mg/kg IV slowly |
| Sodium bicarbonate | Severe metabolic acidosis, hyperkalemia | 1 mEq/kg IV | 1 mEq/kg IV |
| Hydrocortisone | Adrenal insufficiency, bronchospasm | 100 mg IV | 2–4 mg/kg IV (max 100 mg) |
| Labetalol | Hypertensive crisis | 10–20 mg IV over 2 min | 0.2–1 mg/kg IV slowly |
| Salbutamol (Albuterol) | Bronchospasm, hyperkalemia | 2.5 mg nebulized or 100 mcg MDI | 0.15 mg/kg nebulized (min dose 2.5 mg) |
| Dantrolene | Malignant hyperthermia (MH) | 2.5 mg/kg IV, repeat q5–10 min (max 10 mg/kg) | Same as adult |
| Lipid Emulsion 20% | LAST (local anesthetic systemic toxicity) | 1.5 mL/kg IV bolus → 0.25 mL/kg/min infusion | Same as adult |
| Phenylephrine | Hypotension, vasoplegia | 50–200 mcg IV bolus or 0.1–1 mcg/kg/min infusion | 1–2 mcg/kg bolus or infusion |
| Noradrenaline (Norepi) | Vasopressor in shock | 0.05–1 mcg/kg/min infusion | 0.05–1 mcg/kg/min infusion |
| Ketamine | Bronchospasm, induction, sedation | 1–2 mg/kg IV or 4–6 mg/kg IM | 1–2 mg/kg IV or 4–6 mg/kg IM |
| Propofol | Sedation, induction | 1–2 mg/kg IV bolus | 2–3 mg/kg IV bolus |
💡 Low-Resource Pearls:
- No dantrolene? → Cool patient, stop volatile, ICU transfer.
- No lipid rescue? → Early airway, benzodiazepines, basic resuscitation.
- No infusion pumps? → Use manual drip estimation + vigilant monitoring.
1️⃣4️⃣ MCQs — Clinical Scenarios in Perioperative Emergencies
These multiple-choice questions are crafted from real perioperative experiences — designed to reinforce pattern recognition, decision-making, and clinical instinct.
1. Sudden Bradycardia During Spinal
A 26-year-old patient undergoing inguinal hernia repair under spinal anesthesia suddenly becomes bradycardic (HR 35 bpm) and hypotensive.
🧠 What is the FIRST best step?
- A. Administer atropine 0.6 mg IV
- B. Give ephedrine 6 mg IV
- C. Increase IV fluids and tilt table head-down
- D. Start chest compressions
✅ Answer: C
🧠 Explanation: This is likely a high spinal-induced bradycardia. First priority is restoring preload — fluid + position.
2. Intraoperative Bronchospasm in Child
During tonsillectomy, the child suddenly desaturates with chest tightness and wheezing.
🧠 What is the most appropriate next step?
- A. Stop surgery and deepen anesthesia
- B. Administer salbutamol via ETT
- C. Give IV hydrocortisone
- D. All of the above
✅ Answer: D
🧠 Explanation: This is a bronchospasm. Manage with bronchodilator, deepen anesthetic plane, and corticosteroids.
3. Sudden ETCO₂ Drop Post-Hip Surgery
A 52-year-old patient post-hip replacement becomes tachycardic, hypotensive, and shows a sudden drop in ETCO₂ from 35 to 20 mmHg.
🧠 What’s your top diagnosis?
- A. Myocardial infarction
- B. Hypovolemia
- C. Pulmonary embolism
- D. Sepsis
✅ Answer: C
🧠 Explanation: Sudden fall in ETCO₂ + hemodynamic collapse strongly suggests PE.
4. Cyanosis After Lidocaine in G6PD
A patient with G6PD deficiency receives lidocaine infiltration and becomes cyanotic with low SpO₂ not responding to O₂.
🧠 What’s the most likely diagnosis?
- A. Bronchospasm
- B. Methemoglobinemia
- C. Aspiration
- D. Pulmonary embolism
✅ Answer: B
🧠 Explanation: Lidocaine can trigger methemoglobinemia, especially in G6PD patients.
5. Pink Frothy Sputum After Obstruction
Following a difficult intubation and brief airway obstruction, the patient develops hypoxia and pink frothy sputum. CXR: bilateral infiltrates.
🧠 Diagnosis?
- A. Pulmonary embolism
- B. ARDS
- C. Negative pressure pulmonary edema (NPPE)
- D. Aspiration pneumonitis
✅ Answer: C
🧠 Explanation: NPPE follows upper airway obstruction and strong inspiratory effort. Treat supportively.
6. Apnea After Spinal in C-Section
A woman undergoing C-section under spinal suddenly becomes apneic and unresponsive.
🧠 What’s the most likely cause?
- A. High spinal block
- B. Amniotic fluid embolism
- C. Local anesthetic toxicity
- D. Pulmonary embolism
✅ Answer: A
🧠 Explanation: A high spinal can block the phrenic nerve and cause unconsciousness. Always monitor level of block.
7. Confusion & Rash After Femur Surgery
A 24-year-old male develops confusion, tachycardia, hypoxia, and a petechial rash 24 hours after femur fixation.
🧠 Most likely diagnosis?
- A. Fat embolism syndrome
- B. Pulmonary embolism
- C. Aspiration
- D. Anaphylaxis
✅ Answer: A
🧠 Explanation: FES classic triad: Hypoxia, neuro signs, petechiae — commonly post long bone trauma.
8. Masseter Spasm After Sux
Following suxamethonium administration, the patient develops masseter spasm and rising ETCO₂.
🧠 What are you most concerned about?
- A. Seizure
- B. Hypoventilation
- C. Malignant hyperthermia
- D. Myasthenic crisis
✅ Answer: C
🧠 Explanation: Early MH sign. Masseter spasm + hypercapnia = act fast, stop trigger, give dantrolene.
9. Bradycardia During Eye Surgery
A child undergoing strabismus surgery suddenly becomes bradycardic.
🧠 What reflex is triggered?
- A. Oculocardiac reflex
- B. Trigeminal-vagal reflex
- C. Gag reflex
- D. Sympathetic overdrive
✅ Answer: A
🧠 Explanation: Classic OCR: traction on eye muscles → vagal stimulation → bradycardia. Stop pull, give atropine.
10. Bradycardia During Hemorrhoidectomy
A spinalized patient undergoing hemorrhoidectomy develops severe bradycardia and syncope.
🧠 What is the likely trigger?
- A. Blood loss
- B. Drug allergy
- C. Anal stretch / high vagal tone
- D. Local anesthetic toxicity
✅ Answer: C
🧠 Explanation: Anal dilation can provoke intense vagal response. Manage supportively, consider anticholinergic.
11. Rigidity After Fentanyl + Sux
A sedated patient develops trismus, rigidity, and high airway pressures after fentanyl and sux.
🧠 Most likely diagnosis?
- A. Neuroleptic malignant syndrome
- B. Opioid-induced rigidity
- C. Malignant hyperthermia
- D. Seizure
✅ Answer: C
🧠 Explanation: Suspect MH if rigidity + ventilatory issues post trigger drugs. Give dantrolene ASAP.
12. Sudden ETCO₂ = 0, No Chest Rise
During surgery, ETCO₂ drops to 0, SpO₂ falls, and no chest rise is seen.
🧠 First best step?
- A. Give 100% O₂
- B. Check tube placement and patency
- C. Administer bronchodilator
- D. Call for chest x-ray
✅ Answer: B
🧠 Explanation: Always rule out tube kink, dislodgement, or obstruction first in airway crisis.
13. Can’t Intubate, Can’t Oxygenate
During RSI, you can’t intubate, can’t mask ventilate, and SpO₂ is dropping.
🧠 What is the next life-saving action?
- A. Needle cricothyrotomy
- B. Give more suxamethonium
- C. Jaw thrust + mask ventilation
- D. Wait for spontaneous effort
✅ Answer: A
🧠 Explanation: CICO is a surgical airway situation. Go for needle cric or scalpel-bougie-tube.
14. Confusion & Prolonged QT After Transfusion
After massive transfusion, patient is confused. ECG shows prolonged QT.
🧠 What electrolyte abnormality is most likely?
- A. Hyperkalemia
- B. Hypocalcemia
- C. Alkalosis
- D. Hyperglycemia
✅ Answer: B
🧠 Explanation: Citrate in blood products chelates calcium → QT prolongation, hypotension, arrhythmia.
15. Seizure After Local Block
A patient receiving a large volume local block becomes drowsy, then seizes.
🧠 What’s the antidote?
- A. Flumazenil
- B. Dantrolene
- C. Lipid emulsion
- D. Sodium bicarbonate
✅ Answer: C
🧠 Explanation: LAST is managed by IV 20% lipid bolus + infusion. Support airway, seizure control.
1️⃣5️⃣ Final Words
Perioperative emergencies demand not just skill — but clarity in chaos.
This Mastery Guide is your anchor in complexity.
Our goal is to empower clinicians with structure, clarity, and bedside-ready strategies — whether you’re a critical care provider, anesthesia specialist, internist, or medical educator.
From laryngospasm to LAST, from vagal arrest to embolic storms, this guide distills the unthinkable into the manageable, the sudden into the structured.
This guide is your reference when facing perioperative emergencies — in every setting.
Stay structured. Stay vigilant. Act wisely. 🧠
📌 Prepared for Dr. Amir Fadhel – Specialist in Anesthesiology and Critical Care
🗓️ Created: 07/06/2025
🗓️ Last Updated: 08/06/2025
🔗 Explore the Full Mastery Series: Mastery Series in Anesthesia & Critical Care