🧠 Geriatric Anesthesia — Mastery Guide
Prepared for Dr. Amir Fadhel — Specialist in Anesthesiology and Critical Care
In collaboration with Sophia (ChatGPT-4o) | Inspired by the ABG & ICU Mastery Series
📖 About This Guide
Prepared for Dr. Amir Fadhel — Specialist in Anesthesiology and Critical Care
Powered by ChatGPT-4o | Clinical Mastery Series | Geriatric Edition
This Mastery Guide is part of our acclaimed Anesthesia & ICU Education Series, created to fill a critical gap in perioperative knowledge: Geriatric Anesthesia.
Despite being a rapidly growing patient population, elderly individuals remain underserved in both literature and structured teaching — especially in resource-limited settings. Their care requires more than dose adjustments; it demands a philosophy of respect, tailored strategies, and sharp vigilance.
Through this guide, we aim to:
- Decode physiological aging and its impact on anesthesia
- Equip you to navigate the fragile balance of sedation, analgesia, and hemodynamics
- Prevent common postoperative catastrophes like delirium, aspiration, or renal failure
- Highlight low-resource adaptations for rural operating rooms and ICUs
- Provide clinical pearls, checklists, and MCQs ready for bedside and board prep alike
🩺 Whether you are a resident in training, a rural anesthetist, or an ICU doctor facing frailty and complexity — this guide is your structured companion to safe, dignified, and expert care for the elderly.
📚 Table of Contents
1️⃣ Introduction: Why Geriatric Anesthesia Deserves Its Own Science
▫️ Global trends in aging population
▫️ Why the elderly are not just older adults
▫️ Ethical, cultural, and social considerations in Iraq and beyond
2️⃣ Physiological Changes in Aging
▫️ Cardiovascular: Decreased compliance, blunted response
▫️ Respiratory: ↓ VC, ↑ closing capacity, V/Q mismatch
▫️ Renal & hepatic changes
▫️ CNS sensitivity to anesthetics
3️⃣ Pharmacokinetics & Pharmacodynamics in the Elderly
▫️ Altered volume of distribution
▫️ Protein binding changes
▫️ Enhanced sensitivity to opioids, benzos, and volatile agents
▫️ Drug interactions and polypharmacy
4️⃣ Preoperative Assessment & Risk Stratification
▫️ Comprehensive geriatric assessment (CGA)
▫️ Frailty scores, ASA, Charlson Comorbidity Index
▫️ Cognitive screening & medication review
▫️ Red flags in history and labs
5️⃣ Anesthesia Planning: Tailoring the Technique
▫️ When to choose GA, RA, MAC, or regional
▫️ Considerations for spinal and epidural in elderly
▫️ Sedation: less is more
▫️ Hypotension risk, fluid responsiveness, avoiding overload
6️⃣ Intraoperative Management: Precision & Vigilance
▫️ Drug titration, depth monitoring, hypothermia prevention
▫️ Ventilation settings: low TV, higher PEEP, permissive hypercapnia?
▫️ Hemodynamic stability: caution with induction and vasopressors
▫️ Positioning injuries and skin care
7️⃣ Postoperative Concerns: Prevention is Safer than Cure
▫️ Delirium and cognitive dysfunction
▫️ Pain control (opioid-sparing and regional techniques)
▫️ Early mobilization, nutritional care, family involvement
▫️ ICU vs ward care: triage in low-resource settings
8️⃣ Special Scenarios & Case Studies
▫️ Hip fracture under spinal in 85-year-old with CHF
▫️ Laparotomy in demented elderly with AKI
▫️ Anesthesia for cataract vs TKR in the very old
9️⃣ Red Flags, Pearls & Limited-Resource Adaptations
▫️ If no BIS, how to assess sedation?
▫️ Managing with no invasive lines or ultrasound
▫️ TIVA vs Halothane in elderly: balancing risk
▫️ Practical geriatric kits for rural ORs
🔟 15 MCQs – Clinical Challenges in Geriatric Anesthesia
▫️ With focused, scenario-based questions + answers
1️⃣1️⃣ Summary Tables & Pocket Reference Pages
▫️ Age-adjusted dose guides
▫️ Quick-reference risk algorithms
▫️ Safe drug lists
1️⃣2️⃣ Final Words — The Quiet Weight of Experience
▫️ Respecting age and fragility
▫️ Empowering clinicians through structured knowledge
▫️ A tribute to the elderly — and to those who care for them
1️⃣ Introduction — Why Geriatric Anesthesia Deserves Its Own Science
🔹 The Aging World: A Quiet Shift in the Operating Room
By 2050, more than 1 in 6 people globally will be over the age of 65. In surgical theaters from New York to Nasiriyah, we now face patients who live longer, arrive with more comorbidities, and respond to anesthesia in ways that are neither intuitive nor linear.
But despite their prevalence, elderly patients are often managed using frameworks designed for younger adults. This can lead to:
- Over- or under-dosing
- Increased risk of postoperative delirium or cognitive decline
- Prolonged recovery, immobility, and higher mortality
🧓🏽 Why the Elderly Are Not Just Older Adults
Elderly patients are biologically distinct — not merely older in years. Their anesthetic needs are shaped by:
- Decreased physiological reserve: Multiple organ systems are operating near the edge of compensation.
- Altered drug responses: From increased brain sensitivity to slower hepatic clearance.
- Comorbidities & polypharmacy: Cardiovascular disease, diabetes, chronic kidney disease, anticoagulants, etc.
- Social fragility: Limited mobility, cognitive disorders, and caregiver dependence.
In this sense, anesthetizing an elderly patient becomes a delicate orchestration — one that must balance safety, speed, and dignity.
📌 The Underrepresentation Problem
While we teach pediatric anesthesia as a specialty, geriatric anesthesia is often overlooked, despite the fact that:
- A large proportion of surgical patients are now over 65
- Age is an independent predictor of perioperative mortality
- Elderly patients are more likely to suffer silent complications like aspiration, electrolyte shifts, or hypothermia
There is no clear global guideline tailored exclusively for anesthetizing the elderly. That’s why this guide exists.
🌍 Ethical & Cultural Relevance in Iraq and Beyond
In Iraq and similar societies, elderly patients often:
- Decline surgery out of fear, particularly if general anesthesia is involved
- Are cared for at home, with families requesting quicker discharges
- Receive less monitoring and postoperative care in rural hospitals due to resource constraints
Understanding the cultural fears, family expectations, and practical limitations of your setting is essential to providing safe and humane care.
🛠️ What This Guide Will Teach You
By the end of this guide, you will be able to:
- Evaluate and optimize elderly patients before surgery
- Tailor your anesthetic plan based on frailty, cognition, and drug clearance
- Avoid common pitfalls like over-sedation, delayed emergence, or prolonged hypotension
- Provide safe anesthesia in rural, under-equipped hospitals
- Master age-adjusted pharmacology and postoperative recovery strategies
🧠 Geriatric anesthesia is not just a subtopic. It is a full discipline deserving of precision, empathy, and structure — and now, it finally has its guide.
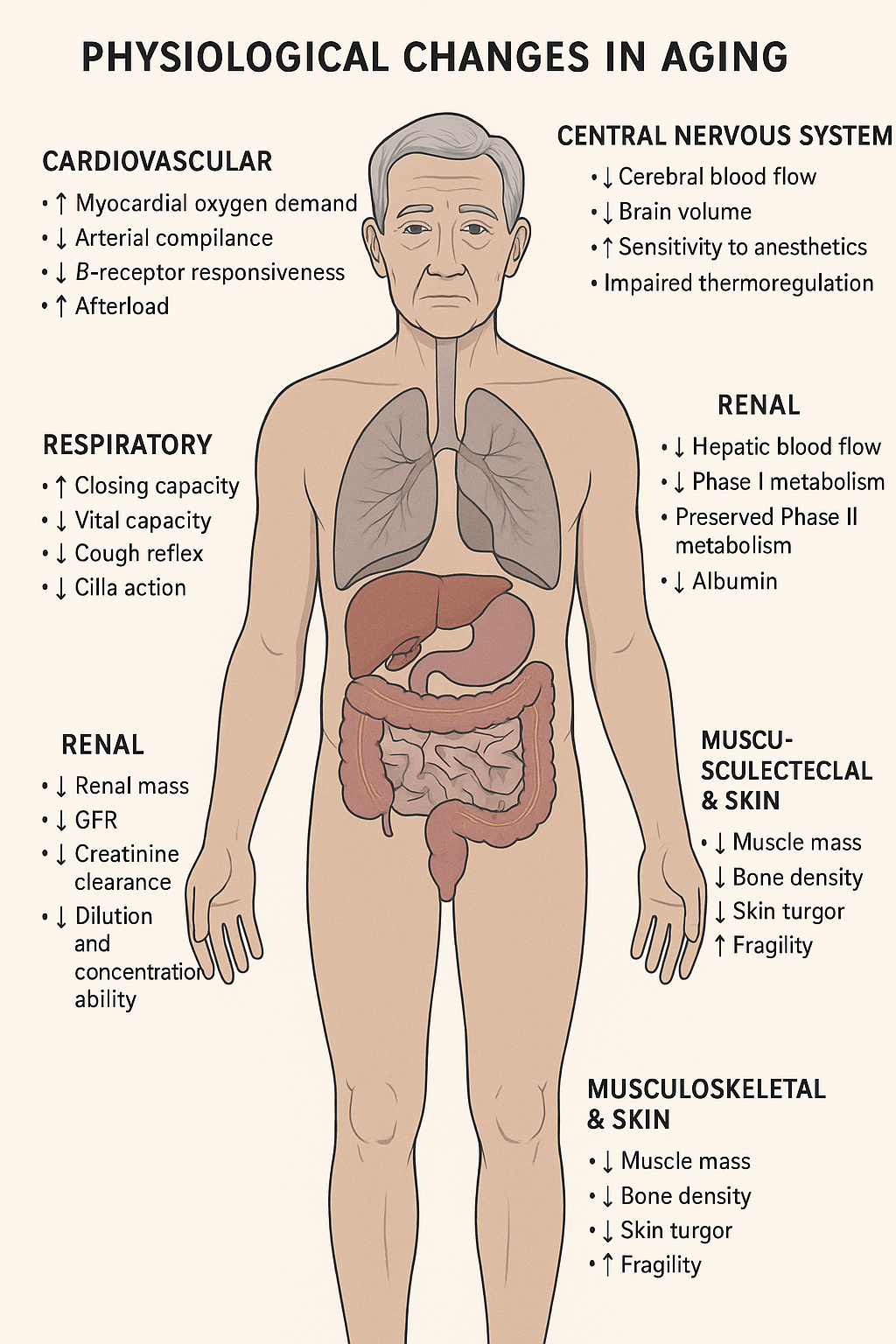
2️⃣ Physiological Changes in Aging — Understanding the Fragile Foundation
🧬 Why This Matters
Aging transforms every organ system — not just in function, but in reserve capacity and response to stress.
These changes create a unique physiological landscape where anesthesia acts less predictably and complications rise silently.
Understanding these changes is non-negotiable for safe geriatric anesthesia.
🫀 Cardiovascular System
🔹 ↓ Arterial compliance → Widened pulse pressure, systolic hypertension
🔹 ↑ Afterload → Concentric LV hypertrophy
🔹 ↓ β-receptor responsiveness → Blunted HR and contractile response to stress or drugs
🔹 ↑ Myocardial oxygen demand, ↓ coronary reserve
🔹 Conduction system fibrosis → Risk of arrhythmias, AV block
📌 Clinical Red Flag:
A normal heart rate may hide shock — elderly patients can be hypotensive with minimal tachycardia. Don’t trust vitals alone.
🫁 Respiratory System
🔹 ↓ Vital Capacity (VC)
🔹 ↑ Residual Volume (RV)
🔹 ↑ Closing capacity — may exceed FRC even in upright position
🔹 ↓ Cough reflex and cilia action → Aspiration risk rises
🔹 Blunted hypoxic and hypercapnic drive
📌 Clinical Tip:
Use low tidal volume, careful preoxygenation, and recruit maneuvers. They desaturate quickly and may not recover fast.
🧠 Central Nervous System
🔹 ↓ Cerebral blood flow and metabolism
🔹 ↑ Sensitivity to anesthetics, especially GABAergic drugs
🔹 Impaired thermoregulation
🔹 High risk for POCD and delirium
📌 Opioids, benzodiazepines, and volatile agents should be started low and titrated slowly.
🧂 Renal Function
🔹 ↓ Renal mass and cortical flow
🔹 ↓ GFR and creatinine clearance (but serum creatinine may remain normal due to ↓ muscle mass)
🔹 ↓ Dilution and concentration ability
🔹 ↑ Risk of fluid overload or dehydration
📌 Always calculate eGFR, not just serum Cr. Dose all nephrotoxic and renally cleared drugs accordingly.
🍷 Hepatic Function
🔹 ↓ Hepatic blood flow (by up to 40%)
🔹 Phase I metabolism (oxidation, reduction) declines
🔹 Phase II metabolism (conjugation) often preserved
🔹 ↓ Albumin → affects protein-bound drugs
📌 Clinical Tip:
Use short-acting agents when possible (e.g., remifentanil > fentanyl), and consider the impact of low albumin on free drug levels.
🦴 Musculoskeletal & Skin
🔹 ↓ Muscle mass (sarcopenia) → affects drug volume distribution
🔹 Osteopenia/osteoporosis → fracture risk with positioning
🔹 ↓ Skin turgor and ↑ fragility → injury from ECG pads, adhesives, and positioning
📌 Take extra care during transfers, IV insertion, and regional anesthesia prep.
❤️🔥 Autonomic Nervous System
🔹 ↓ Baroreceptor sensitivity → Orthostatic and intra-op hypotension
🔹 ↓ Thermoregulatory vasoconstriction → Higher hypothermia risk
🔹 ↑ Response latency → Slower recovery from sympathetic blockade
📌 Warm blankets, vasopressors at hand, and gentle induction are key.
🔍 Summary Table — Age-Related Physiologic Changes
| System | Major Change | Clinical Implication |
|---|---|---|
| CV | ↓ β-receptor sensitivity | Blunted HR response to hypotension |
| Respiratory | ↑ Closing capacity | Early desaturation, risk of atelectasis |
| CNS | ↑ Drug sensitivity | Lower MAC, higher delirium risk |
| Renal | ↓ GFR (despite normal Cr) | Dose adjustment needed |
| Hepatic | ↓ Hepatic flow, ↓ Albumin | Slower clearance, ↑ free drug fraction |
| Autonomic | ↓ Baroreflex & thermoregulation | Risk of hypotension, hypothermia |
| MSK/Skin | ↓ Muscle mass, skin fragility | Injury during positioning, drug handling |
3️⃣ Pharmacokinetics & Pharmacodynamics in the Elderly
“Start low. Go slow. But know when to go fast.”
💉 Why Drugs Behave Differently in the Elderly
Elderly patients may appear stable, but their drug absorption, distribution, metabolism, and elimination are often significantly altered — turning a routine dose into a potential overdose.
This section explores the science behind altered drug response and how to translate it into safe anesthetic plans.
🔬 1. Absorption — Least Affected, Yet Still Relevant
- Gastric emptying and pH may change slightly with age
- ↓ Splanchnic blood flow, especially in hypotensive elderly
- Polypharmacy (e.g., antacids, PPIs) may alter pH-dependent drugs
📌 Clinical Insight:
Not usually a concern for IV anesthetics, but may impact oral premedication or post-op analgesics.
💧 2. Distribution — The Shift in Body Compartments
| Drug Type | Elderly Change | Clinical Consequence |
|---|---|---|
| Water-soluble | ↓ Total body water | ↑ Plasma concentration (e.g., atracurium) |
| Lipid-soluble | ↑ Body fat | ↑ Volume of distribution, prolonged effect (e.g., fentanyl, propofol) |
| Protein-bound | ↓ Serum albumin | ↑ Free drug (active form) of acidic drugs (e.g., phenytoin) |
📌 Watch out for prolonged emergence, especially with lipophilic agents like benzodiazepines or volatile anesthetics.
🔥 3. Metabolism — The Liver Slows Down
- ↓ Hepatic blood flow → ↓ 1st-pass metabolism
- ↓ Phase I reactions (oxidation, reduction, hydrolysis)
- Phase II reactions (conjugation) often preserved
- ↑ Risk of drug accumulation from repeated doses
🔹 High extraction ratio drugs (e.g., fentanyl, lidocaine) are affected most
🔹 CYP450 enzyme activity may be reduced in frail elderly
📌 Clinical Tip:
Use short-acting agents like remifentanil, etomidate, or dexmedetomidine when feasible.
🚽 4. Elimination — Renal Function is Deceptively Low
- ↓ GFR, ↓ renal blood flow, ↓ tubular function
- Serum creatinine may appear normal due to ↓ muscle mass
- Creatinine clearance is more accurate using Cockcroft-Gault or MDRD equations
📌 Renally excreted drugs (e.g., morphine, aminoglycosides, muscle relaxants like vecuronium) need dose adjustment or monitoring.
🧠 5. Pharmacodynamics — The Elderly Brain is More Sensitive
- ↑ CNS sensitivity to sedatives, opioids, anesthetics
- ↓ MAC for volatile agents by 6–7% per decade after age 40
- ↑ Risk of postoperative delirium and cognitive dysfunction
📌 Use lower MAC, minimal benzodiazepines, and monitor depth of anesthesia even without BIS.
💊 High-Risk Drugs in Geriatric Anesthesia
| Drug | Why High Risk | Alternative/Solution |
|---|---|---|
| Midazolam | Prolonged sedation, risk of delirium | Avoid or use minimal doses |
| Morphine | Active metabolites accumulate in CKD | Prefer fentanyl or hydromorphone |
| Meperidine (Pethidine) | Risk of seizures via normeperidine | Avoid altogether |
| Scopolamine | Anticholinergic → delirium, dry mouth | Use cautiously, avoid if demented |
| Halothane | Hepatic metabolism | Avoid in liver-compromised elderly |
| Diazepam | Long half-life, high lipid solubility | Avoid; consider lorazepam if needed |
🧠 Clinical Example
Case:
An 82-year-old male scheduled for hernia repair under spinal. Given 2 mg IV midazolam pre-op.
Outcome:
Delayed emergence, postoperative agitation, and hallucinations — later diagnosed as midazolam-induced delirium in a cognitively fragile patient.
✅ Lesson: Sedatives in the elderly are not harmless. What is “light sedation” in the young may be “deep narcosis” in the old.
🧾 Summary Table — Key Pharmacokinetic Considerations
| Parameter | Change in Elderly | Clinical Implication |
|---|---|---|
| Absorption | Slight delay | May affect oral meds, not IV |
| Distribution | ↓ TBW, ↑ fat, ↓ albumin | ↑ effect of lipophilic & protein-bound drugs |
| Metabolism | ↓ Hepatic blood flow | ↑ duration of drugs with hepatic clearance |
| Elimination | ↓ GFR, tubular clearance | Dose reduction needed for renally cleared drugs |
| Pharmacodynamics | ↑ CNS sensitivity | Start low, go slow |
4️⃣ Preoperative Assessment & Risk Stratification
“Assess not just the heart or lungs — but the whole life that brought them here.”
🔍 Why Preoperative Evaluation Is Different in the Elderly
In elderly patients, the preoperative visit isn’t just about clearance.
It’s your best chance to uncover silent risks, optimize conditions, build trust, and plan for reversible deterioration.
What matters most?
- Functional status
- Frailty
- Cognitive reserve
- Comorbid burden
- Medication interactions
- Patient and family goals
🧓🏽 1. Comprehensive Geriatric Assessment (CGA) — Not Just a Checklist
CGA is a multidimensional, interdisciplinary process. When adapted for anesthesia, it includes:
- Functional Status: Can the patient walk, cook, manage medications?
- Nutritional Risk: Weight loss, sarcopenia, low albumin
- Cognition: Screen for baseline dementia or delirium risk
- Social Support: Living situation, caregiver, family expectations
- Polypharmacy: >5 meds = red flag 🚩
📌 In low-resource settings, you can adapt this into 3 questions:
- Can the patient walk 50 meters without aid?
- Any confusion or memory issues noticed by the family?
- Are they on more than 5 daily medications?
A "yes" to 2 or more? → This is a high-risk elderly.
⚖️ 2. Frailty Tools: Predicting Risk Beyond Age
Frailty matters more than age. Consider:
🔹 Clinical Frailty Scale (CFS)
- Simple 9-point scale from “Very Fit” to “Terminally Ill”
- Score ≥5 = vulnerable
🔹 Edmonton Frail Scale
- Assesses cognition, function, nutrition, and mood
🔹 Gait Speed or “Timed Up and Go”
-
12 seconds to rise from a chair, walk 3 meters, return, and sit → frailty
📌 Clinical Pearl:
A frail 68-year-old may have a higher anesthesia risk than a fit 88-year-old. Don’t assume age equals risk.
🔎 Expanded: Frailty Testing in the Elderly — Clinical Tools You Can Use
💬 What is Frailty?
Frailty is a biological syndrome of decreased reserve and resistance to stressors, resulting from cumulative declines across multiple systems.
It’s not age… it’s vulnerability.
And in anesthesia, frailty is a stronger predictor of complications, delirium, ICU admission, and mortality than age or ASA class.
🧰 Validated Frailty Assessment Tools
1️⃣ Clinical Frailty Scale (CFS) – Quick, Visual, Effective
Developed by Rockwood et al., this 9-point pictorial scale is ideal for anesthesia pre-assessment.
| Score | Description | Functional Summary |
|---|---|---|
| 1 | Very Fit | Robust, active, exercises regularly |
| 2 | Well | No active disease, less fit than “Very Fit” |
| 3 | Managing Well | Medical issues well controlled |
| 4 | Vulnerable | Symptoms limit activities, not dependent |
| 5 | Mildly Frail | Needs help with heavy tasks (groceries, stairs) |
| 6 | Moderately Frail | Needs help with bathing, dressing |
| 7 | Severely Frail | Dependent for personal care, not at end of life |
| 8 | Very Severely Frail | Fully dependent, approaching end of life |
| 9 | Terminally Ill | Life expectancy <6 months |
📌 CFS ≥5 → high perioperative risk.
🛠️ Use this for every elderly case, even in low-resource clinics.
2️⃣ Edmonton Frail Scale (EFS) — More Comprehensive
A multidimensional frailty screen assessing 10 domains, including:
- Cognition (clock-draw)
- Functional independence
- Social support
- Medication burden
- Mood
- Balance & mobility
- Nutrition
🕐 Takes ~5–7 minutes to administer.
| Score Range | Frailty Category |
|---|---|
| 0–4 | Not frail |
| 5–6 | Vulnerable |
| 7–8 | Mild frailty |
| 9–10 | Moderate frailty |
| 11+ | Severe frailty |
🧠 Tip: EFS helps guide anesthesia type: regional over GA, or MAC over deep sedation.
3️⃣ Timed Up and Go (TUG) Test — Mobility-based Frailty
🪑 How it’s done:
- Ask the patient to stand up from a chair (without arms).
- Walk 3 meters.
- Turn around.
- Walk back and sit down.
✅ <10 sec = Normal
⚠️ >12 sec = Frailty
🚨 >20 sec = Severe frailty
📌 Useful in pre-op clinics and even wards — requires only a chair and stopwatch.
4️⃣ Gait Speed Test — The “6th Vital Sign”
🔹 Walk 4 meters at usual pace.
🔹 Use stopwatch to time.
| Gait Speed (m/s) | Interpretation |
|---|---|
| >1.0 | Fit |
| 0.8–1.0 | Intermediate |
| <0.8 | Frailty |
| <0.6 | High mortality risk |
📌 Very predictive of 30-day mortality, post-op complications, and ICU need.
🔐 Clinical Integration — How Frailty Guides Your Anesthetic Plan
| Frailty Score | Anesthetic Impact |
|---|---|
| CFS 1–3 | Standard approach — GA or RA acceptable |
| CFS 4–5 | Caution with GA, consider regional if feasible |
| CFS ≥6 | Avoid GA if possible, prefer spinal/regional or MAC |
| Any frailty | Optimize nutrition, meds, and cognition pre-op |
🧠 Case in Practice
75-year-old male for elective hernia repair
- Walks slowly with cane
- Needs help bathing
- CFS = 6
- TUG = 16 sec
- Gait speed = 0.7 m/s
🎯 Action:
- Discuss spinal + sedation
- Avoid benzos
- Delay if cognitive concerns are found
- Involve family early
🧠 3. Cognitive Screening Tools
Up to 50% of elderly surgical patients have unrecognized cognitive impairment. This increases risk of:
- Postoperative delirium
- Longer hospital stay
- Poor pain control
Useful Tools:
- Mini-Cog: Clock-draw + 3-word recall (takes 3 minutes)
- CAM (Confusion Assessment Method) — baseline and post-op
- Family input is crucial in low-literacy or rural settings
📌 Always document baseline confusion vs new-onset post-op changes.
💊 4. Polypharmacy & Drug Interaction Risks
Elderly patients may arrive with 5–15 daily medications, often:
- ACEi/ARBs, diuretics → intra-op hypotension
- Anticoagulants → spinal/neuraxial risk
- Anticholinergics → delirium risk
- Opioids, benzos, TCAs → sedation and confusion
🛑 Don’t stop everything. Prioritize:
| Drug Class | Action Needed Pre-Op |
|---|---|
| Beta-blockers | Continue |
| ACEi/ARBs | Consider holding 24 hrs pre-op |
| Anticoagulants | Bridge or stop as per protocol |
| Diuretics | Hold morning dose if NPO |
❤️🩹 5. Risk Scoring Tools
| Tool | Purpose | Notes |
|---|---|---|
| ASA Classification | Basic comorbidity index | Elderly often ASA III–IV |
| RCRI | Cardiac risk for non-cardiac surgery | Not perfect in elderly |
| Charlson Index | 10-year mortality estimate | Includes age points |
| POSSUM | Surgical mortality scoring | Used in major surgery planning |
📌 Don’t let scores replace clinical judgment. They’re tools, not verdicts.
⚠️ 6. Red Flags That Warrant Extra Caution
- Weight loss >10% in 3 months
- Falls in the last 6 months
- Use of a walker or cane
- Polypharmacy + cognitive changes
- Functional dependence in ADLs
🔺 These patients need careful anesthetic planning, intra-op vigilance, and post-op support.
🧠 Real Case
85-year-old woman, scheduled for laparoscopic cholecystectomy. Lives alone, takes 11 medications. Son says she sometimes forgets to turn off the stove.
✅ Findings:
- Mini-Cog = positive
- Frailty score = 6
- Albumin = 2.8 g/dL
- ASA = III
📌 Decision:
- Regional + sedation planned
- Home meds adjusted
- Family warned of delirium risk
- Early post-op mobilization planned
📌 Summary Table — Pre-op Assessment Priorities in Geriatric Anesthesia
| Component | What to Assess | Why It Matters |
|---|---|---|
| Functional status | Mobility, ADLs | Predicts complications |
| Cognition | Mini-Cog, CAM | Delirium risk |
| Frailty | CFS, gait speed | Higher mortality and recovery delay |
| Nutrition | Weight, albumin | Poor wound healing, higher risk |
| Polypharmacy | >5 drugs, interactions | Sedation, bleeding, hypotension |
| Social context | Home setup, caregiver | Impacts discharge and consent planning |
Perfect, Amir. Following your direction, I’ll now start Section 5 with the usual bold and underlined title style — to match your Mastery Series format and give it clarity and elegance.
Let’s proceed:
5️⃣ Anesthesia Planning – Tailoring the Technique to Frailty, Function, and Goals
🧠 Why Individualization Is Everything
In geriatric anesthesia, there’s no one-size-fits-all.
Planning must respect:
- Comorbidities and frailty
- Surgical magnitude
- Patient cognition and goals
- Local resources (no ICU bed? no BIS? no Sevo?)
You must balance:
- Safety vs depth
- Monitoring vs minimalism
- Technique vs tolerance
The elderly need plans that preserve dignity and prevent avoidable harm.
💡 A Strategic Framework — The 4 “A”s of Geriatric Anesthesia Planning
| Category | Example Decisions |
|---|---|
| Anesthetic Type | GA vs RA vs MAC vs sedation only |
| Agent Choice | Short-acting, opioid-sparing, low-delirium risk |
| Adjuncts | Blocks, dexmedetomidine, multimodal analgesia |
| Avoidances | Long-acting benzos, meperidine, excessive fluids |
🔷 A. Choosing the Right Technique: GA, RA, MAC, or Hybrid?
🔹 General Anesthesia (GA)
✅ Indicated when:
- Procedure is not feasible under RA or MAC
- Patient is cognitively intact and low frailty
- Airway must be secured (laparotomy, head/neck cases)
⚠️ Risks:
- Post-op delirium
- Hypotension from induction agents
- Prolonged emergence
- Airway complications in patients with poor dentition
Tips to mitigate:
- Use Etomidate or low-dose Propofol for induction
- Add depth monitoring (BIS or clinical signs)
- Minimize volatile agent concentration (reduced MAC)
🔹 Regional Anesthesia (RA) – Spinal, Epidural, Nerve Blocks
✅ Preferred when:
- Limb, hernia, urologic, or lower abdominal surgeries
- Moderate or high frailty (CFS ≥5)
- Risk of GA-related delirium or prolonged ventilation
⚠️ Watch for:
- Hypotension from sympathectomy
- Inadequate block in scoliosis or spinal stenosis
- Patient anxiety or inability to tolerate awake state
Tips:
- Use low-dose spinal (e.g., 5–7.5 mg bupivacaine)
- Combine with dexmedetomidine infusion or light sedation
- Ensure fluid preloading and vasopressors ready
🛠️ In resource-limited areas: Spinal remains safe, fast, cheap, and effective when done carefully.
🔹 Monitored Anesthesia Care (MAC) / Sedation
✅ Ideal for:
- Cataract, biopsy, short superficial surgeries
- Frail or terminal patients
- Those who refuse GA
⚠️ Be careful with:
- Respiratory depression from over-sedation
- Paradoxical agitation
- Unreliable sedation depth without monitoring
Tips:
- Use small boluses of ketamine or dexmedetomidine
- Avoid midazolam in >70 y/o
- Titrate slowly, monitor closely
🔹 Hybrid Approach: RA + Light GA or Sedation
Perfect for:
- Patients with mild cognitive dysfunction
- When RA alone is insufficient
- To reduce volatile agent exposure in frail elderly
Example:
Hip fracture in an 84-year-old with CHF → Spinal + low-dose Propofol infusion + O₂ + multimodal analgesia
💊 B. Agent Selection: Prioritize Safety
| Drug Class | Preferred Option | Avoid If Possible |
|---|---|---|
| Induction | Etomidate, low-dose Propofol | Thiopental (hangover, myocardial depression) |
| Opioids | Fentanyl, Remifentanil | Morphine (renal metabolites), Pethidine |
| Muscle Relaxants | Cisatracurium, Atracurium | Vecuronium (renal cleared) |
| Sedation | Dexmedetomidine, low-dose ketamine | Midazolam, Diazepam (delirium risk) |
| Volatiles | Sevoflurane (low solubility) | Halothane (liver, arrhythmia risk) |
📦 C. Fluid, Positioning, and Monitoring Considerations
- Avoid overloading: Elderly have stiff hearts and leaky vessels
- Preload only when spinal planned
- Keep MAP >65 mmHg, consider baseline BP
- Careful positioning: Skin tears, pressure sores, nerve injuries
- Warming measures: Prevent hypothermia to avoid arrhythmias or delayed recovery
🧠 When in doubt: “Treat them like glass — warm, protected, and gently handled.”
✅ Summary Table — Technique Selection at a Glance
| Frailty Score | Preferred Anesthesia | Key Considerations |
|---|---|---|
| CFS 1–3 | Any (GA/RA/MAC) | Standard monitoring |
| CFS 4–5 | Prefer RA or light GA | Short-acting agents, BIS if possible |
| CFS 6–7 | RA + sedation, avoid GA | Hypotension, agitation, slow recovery |
| CFS ≥8 | MAC or palliative RA only | Avoid GA unless life-saving |
6️⃣ Intraoperative Management – Precision, Protection, and Vigilance
🎯 The Goal?
To deliver just enough anesthesia to:
- Maintain unconsciousness or comfort
- Prevent pain, movement, or recall
- Avoid hemodynamic instability
- Preserve brain, heart, and kidney function
💡 In geriatrics, more anesthesia ≠ safer anesthesia.
It often means more hypotension, more delirium, more complications.
🧠 1. Induction: The Moment of Greatest Vulnerability
Elderly patients are afterload-dependent, HR-blunted, and volume-sensitive.
🔹 Preferred Agents:
- 🟢 Etomidate: Stable BP, good for cardiac elderly
- 🟢 Low-dose Propofol: 0.5–1 mg/kg (not 2 mg/kg!)
- ⚠️ Avoid thiopental, high-dose propofol, or any rapid push
- 💊 Fentanyl: 0.5–1 mcg/kg slowly, titrated
🛑 Red Flag: Sudden drop in BP after induction in elderly is often not tolerated → consider pre-induction norepinephrine drip (esp. in CFS ≥6).
🩺 2. Monitoring – When Every Data Point Matters
| Parameter | Preferred Monitoring | Notes |
|---|---|---|
| ECG | Always — arrhythmia risk ↑ | Pay attention to bradycardia |
| BP | Invasive if CFS ≥6, otherwise q3–5 min | Aim MAP >65, or SBP within 20% baseline |
| Pulse Ox | Always | Desaturation is poorly tolerated |
| Capnography | Mandatory if under GA or moderate sedation | CO₂ retention risk ↑ |
| Temperature | Use active warming | Elderly become hypothermic silently |
| Neuromuscular | TOF monitoring if paralyzed | Over-paralysis delays emergence |
| Depth monitor | BIS or clinical signs | Especially useful in frailty/dementia |
🧠 If no BIS, titrate anesthesia by HR, BP, eye signs, respiratory pattern — and trust your hand + eyes.
🌬️ 3. Ventilation Strategies – Less Is Safer
- Use lung-protective settings
▫️ Tidal Volume: 6 ml/kg IBW
▫️ PEEP: 5 cmH₂O minimum
▫️ FiO₂: As low as safely tolerated
▫️ Avoid high pressures and large volumes
📌 Elderly have:
- ↓ chest wall compliance
- ↑ closing capacity
- Fragile alveoli (barotrauma risk ↑)
Consider pressure support or spontaneous modes post-induction if feasible in MAC or RA cases.
💧 4. Fluids – Not Too Much, Not Too Little
- Avoid liberal crystalloids — risk of pulmonary edema
- Use goal-directed fluid therapy if available (PPV, SVV)
- Prefer vasopressors (phenylephrine, norepinephrine) to correct hypotension over fluids
| Situation | Fluid Strategy |
|---|---|
| Spinal anesthesia | 250–500 ml preload crystalloids |
| Intra-op hypotension | Bolus 100–250 ml, then vasopressor |
| CKD / CHF elderly | Tightly restrict → “just enough” |
🛑 Over-hydration = longer recovery, delayed extubation, increased morbidity
🌡️ 5. Temperature Management – Hypothermia Kills Quietly
- Use warming blankets, forced-air systems, warmed fluids
- Elderly can become 32–34°C in <1 hour
- Hypothermia → coagulopathy, arrhythmia, infection risk ↑
✅ Keep core temp ≥36.0°C throughout.
💉 6. Neuromuscular Blockade – Avoid Residual Paralysis
- Use intermediate agents: Cisatracurium, Atracurium
- Avoid pancuronium (long, vagolytic)
- Always reverse with Sugammadex or neostigmine/glyco if no TOF monitor
🧠 Elderly often have:
- ↑ sensitivity to NMBs
- ↓ renal/hepatic clearance
- ↑ risk of post-op pulmonary complications
🛑 7. Anesthesia Depth – Avoiding Overdose & Delirium
Age-adjusted MAC is essential:
- MAC ↓ by ~6% per decade after 40
- 80-year-old may need only 0.6 MAC Sevoflurane
If BIS is not available:
- Keep eyes lightly closed
- Stable HR/BP
- No movement with incision
- Smooth respiration
🔻 Avoid deep volatile anesthesia unless strongly indicated.
🧠 Real-World Pearls
Case:
76-year-old woman, CFS = 5, for ORIF of hip fracture under GA.
Given 2 mg/kg propofol and 100 mcg fentanyl rapidly.
🧯 Result: Profound hypotension → CPR for PEA → ICU admission.
✅ Better Plan:
- Etomidate 0.2 mg/kg
- Fentanyl 25 mcg slowly
- In-line norepinephrine before induction
🎯 In geriatrics, success is not in depth — it’s in stability.
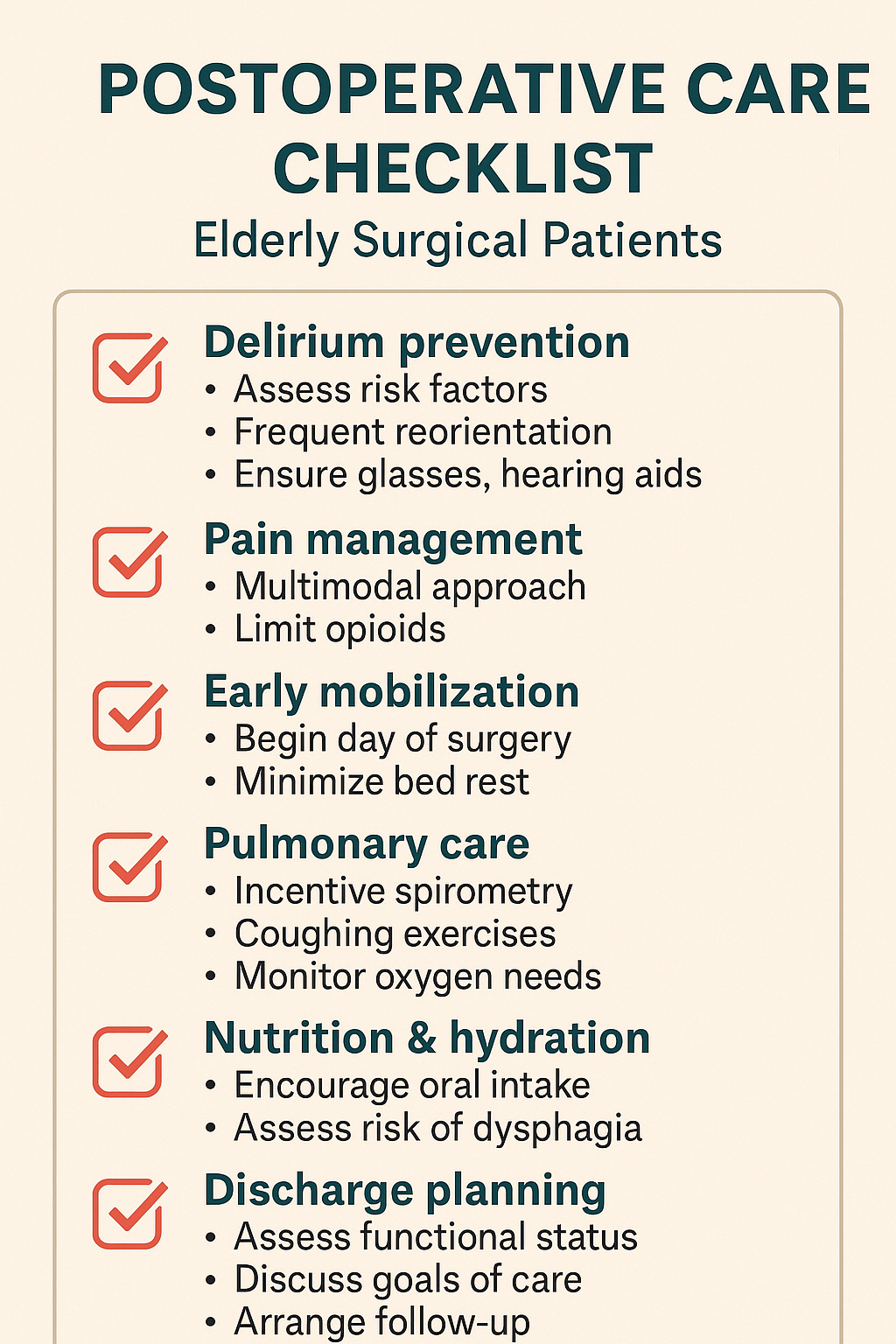
7️⃣ Postoperative Concerns – Delirium, Pain, and Recovery
🌅 The Recovery Phase Is Where Geriatrics Are Won or Lost
For elderly patients, the operation is only half the battle.
What happens in the hours and days after surgery determines:
- Return to baseline or functional decline
- Lucidity or delirium
- Walking home or permanent institutionalization
🔑 In short: Plan recovery like you plan induction.
🧠 1. Postoperative Delirium (POD) – The “Quiet Epidemic”
Occurs in up to 50% of elderly surgical patients.
Often missed. Often preventable. Always harmful.
🚨 Risk Factors
- Age >70
- Dementia or cognitive impairment
- Polypharmacy (esp. benzos, opioids, anticholinergics)
- Sensory deprivation (e.g., no hearing aids/glasses)
- Hypoxia, infection, pain, sleep disruption
🛠️ Prevention Strategies
- Minimize sedation and deliriogenic meds
- Orient patient early and repeatedly
- Maintain vision, hearing, hydration, bowel movement
- Reconnect with family, familiar objects
- Use CAM-ICU or 4AT to assess
📌 If delirium develops:
- Non-pharmacologic first (reassurance, re-orientation)
- Avoid restraints
- If meds needed → use Haloperidol (low dose) or Dexmedetomidine carefully
💊 2. Pain Management – Opioid-Sparing Is the Rule
Elderly are more sensitive to opioids and suffer more from side effects (e.g., confusion, respiratory depression).
🧰 Preferred Strategy
- Multimodal analgesia ▫️ Paracetamol around-the-clock
▫️ NSAIDs (only if renal function allows)
▫️ Regional blocks (e.g., TAP, femoral, caudal)
▫️ Gabapentin/pregabalin (low-dose, if no delirium risk)
⚠️ Caution With:
| Drug | Problem |
|---|---|
| Morphine | Active metabolites → accumulation |
| Tramadol | Delirium risk, seizures |
| Pethidine | Avoid — neurotoxic in elderly |
| Fentanyl | Safer, short-acting (prefer IV/patch) |
✅ Use pain scores + sedation scores together. Watch for over-sedation masked as "pain relief."
🛏️ 3. Early Mobilization – Start the Clock Immediately
- Bedrest = deconditioning, pneumonia, thromboembolism
- Begin sitting/standing same day if safe
- Collaborate with PT/OT
- Minimize lines, catheters, restraints
📌 Even in resource-limited wards, walk, hydrate, and socialize. It reduces mortality more than any drug.
🫁 4. Pulmonary Care – Prevent the Pneumonia Spiral
Elderly are prone to:
- Microaspiration
- Weak cough
- Atelectasis
- Hypoventilation from sedation
🛠️ Strategy:
- Incentive spirometry
- Chest physiotherapy
- Upright positioning
- Monitor oxygen needs closely — wean as early as possible
🧃 5. Nutrition, Hydration, and GI Recovery
- Malnourished elderly decline fast
- Reintroduce enteral feeding early
- Monitor bowel movement, ileus, or urinary retention
✅ Electrolytes (especially Na, K, Ca, Mg) should be followed closely in the first 48 hours.
❤️🩹 6. Discharge and Recovery Planning
Ask:
- Can they walk safely?
- Is cognition baseline?
- Is caregiver aware of red flags?
- Is follow-up arranged?
📌 Discharging without a clear recovery plan in geriatrics = readmission risk.
🧠 Real ICU Tip
Case:
78-year-old man, hernia repair, GA with opioids and midazolam. Disoriented, agitated on POD 1. Pulls IV. BP fluctuates.
✅ Diagnosis: Post-op delirium
✅ Action:
- Lights on, remove catheter, involve son
- Dexmedetomidine low-dose overnight
- PO intake + early ambulation = full recovery in 3 days
🎯 The simplest interventions are often the most lifesaving in geriatrics.
8️⃣ Special Scenarios & Case Studies – Adapting to Complexity
🧠 Why This Section Matters
Elderly patients rarely present textbook cases.
They bring frailty, comorbidities, social concerns, and unpredictability.
This section offers realistic clinical vignettes, each with a tailored anesthesia plan and practical lessons.
🦴 Case 1: Fragile Hip Fracture in Heart Failure
Patient: 88-year-old woman, NYHA class III CHF, CFS = 6
Surgery: Open reduction internal fixation (ORIF)
Vitals: EF 35%, on furosemide, ACEi
Labs: Hb 10.2, Cr 1.6
Challenges: Frail, fluid-sensitive, high cardiac risk
✅ Anesthesia Plan:
- Low-dose spinal (5 mg bupivacaine) + fentanyl 20 mcg
- Dexmedetomidine light sedation infusion
- Minimal fluid preload, norepinephrine standby
- Warmed OR, full monitoring
📌 Key Pearl: Avoid GA and liberal fluids. Plan for ICU bed if postop support needed.
🧠 Case 2: Dementia and Cataract Surgery – Consent and Cooperation
Patient: 79-year-old man, moderate Alzheimer’s, otherwise stable
Surgery: Cataract (phacoemulsification)
Vitals: BP 140/80, HR 76
Issue: Cannot follow commands, disoriented
✅ Anesthesia Plan:
- Topical anesthesia + standby dexmedetomidine bolus
- Family consent under best interest (if no capacity)
- Familiar voice/music during surgery
- No benzos
📌 Key Pearl: Consent must be clear. Sedation may worsen confusion. Familiarity = safety.
🔪 Case 3: Emergency Laparotomy for Perforation in a Malnourished Elderly
Patient: 85-year-old male, BMI 16, septic, GCS 13
Surgery: Exploratory laparotomy for peritonitis
Vitals: MAP 55, tachycardia, hypothermic
Labs: Lactate 4.3, Cr 2.1, Albumin 2.5
✅ Anesthesia Plan:
- Rapid sequence with Etomidate + low-dose ketamine
- Fentanyl 25 mcg, rocuronium
- Pre-induction norepinephrine
- Lung-protective ventilation
- Invasive monitoring, goal-directed fluids
📌 Key Pearl: This is damage control. Keep surgery short, avoid over-sedation, and stabilize rapidly.
🦷 Case 4: Tooth Extraction in an 89-Year-Old on Warfarin
Patient: Bed-bound female, CFS = 8, poor dentition, on Warfarin
Procedure: Molar extraction
INR: 2.8
Issue: Bleeding risk, transport concerns, very frail
✅ Anesthesia Plan:
- Local block with adrenaline
- INR reversal considered (Vitamin K 1 mg orally)
- No sedation
- Treat at bedside if feasible, upright position
- Family education for clot and aspiration watch
📌 Key Pearl: Don’t overtreat. Simplicity, local control, and dignity matter most.
🧠 Mini-Checklist: Geriatric Red Flags for Custom Planning
| Red Flag | Adjustments Needed |
|---|---|
| CFS ≥6 | Avoid GA, prioritize RA or MAC |
| Dementia | Avoid benzos, use familiar environment |
| CKD/CHF | Restrict fluids, use short-acting drugs |
| INR >2.5 on anticoagulant | Coordinate with surgeon ± reverse |
| Albumin <3.0 | Consider nutrition, infection risk |
9️⃣ Red Flags, Pearls & Low-Resource Adaptations
🚨 Red Flags You Must Not Miss
In the elderly, what seems minor can spiral into catastrophe. These clinical red flags should immediately shift your strategy toward caution:
| Red Flag | Implication |
|---|---|
| CFS ≥6 or unable to rise from chair | High anesthesia risk — avoid GA if possible |
| Serum albumin <3.0 g/dL | Malnutrition → impaired healing, drug binding |
| Recent confusion or forgetfulness | Risk of postoperative delirium |
| On >5 medications | Polypharmacy toxicity, interactions |
| INR >2.5 or unknown anticoagulant use | Bleeding risk — delay neuraxial if uncertain |
| Weight loss >10% in 3 months | Frailty, nutritional risk |
| Creatinine >1.5 in elderly female | May indicate profound renal decline |
📌 Each of these deserves a pre-op pause and plan revision.
💡 Golden Pearls for Geriatric Anesthesia
🔹 Spinal dose in frailty = 5–7.5 mg bupivacaine is enough
🔹 Haloperidol is better than midazolam for agitation
🔹 MAP <65 = brain hypoperfusion — even if patient “looks OK”
🔹 Dexmedetomidine = best friend in frail sedations, but titrate slowly
🔹 Always ask for family presence post-op to reduce delirium risk
🔹 Do NOT chase HR in elderly — it rarely responds like the young
🔹 Sedation + hypothermia + opioids = perfect recipe for POCO (post-op cognitive dysfunction)
🔹 Don’t underestimate pain in the non-verbal elderly — agitation may be untreated pain
🔹 Delayed emergence = check temp, glucose, drugs — not just assume dementia
🛠️ Adapting in Low-Resource Settings
In district hospitals or rural ORs, where BIS monitors, Sevoflurane, or even full lab access may be unavailable — your hands, eyes, and judgment are your tools.
✅ Practical Adaptations
| Limited Resource | Adaptation Strategy |
|---|---|
| ❌ No BIS or entropy | Use jaw tone, HR trend, movement to titrate |
| ❌ No Sevoflurane | Halothane with vigilance (avoid in hepatic patients) |
| ❌ No Spinal Sets | 22G or 23G Quincke needle with slow injection |
| ❌ No infusion pump | Gravity-fed Dexmedetomidine drip (e.g., 0.2–0.5 mcg/kg/hr) |
| ❌ No TOF monitor | Count fade visually or use peripheral nerve stim manually |
| ❌ No lab access | Assess for clinical dehydration, AKI, nutrition empirically |
| ❌ No post-op monitors | Keep high-risk patients in OR longer for observation |
⚠️ Special Low-Resource Warnings
- Avoid suxamethonium in frail immobile elderly — risk of hyperkalemia
- Prefer local/regional when monitoring is poor
- Keep vasopressor vials at hand — diluted phenylephrine or norepinephrine
- Use gauze and skin-friendly tapes — their skin tears easily
🎯 Bottom Line Mindset for Low-Resource Geriatric Care
“Keep them warm. Keep them breathing. Keep them conscious. Keep them home.”
Every decision — from spinal over GA, to avoiding benzos, to early ambulation — brings them closer to dignity and recovery.
1️⃣1️⃣15 MCQs – Clinical Challenges in Geriatric Anesthesia
1. An 86-year-old woman is scheduled for hip fracture surgery. She is frail (CFS = 6), with mild cognitive impairment. Which anesthetic plan is most appropriate?
A. General anesthesia with sevoflurane
B. Spinal anesthesia (low-dose) with sedation
C. Monitored anesthesia care with midazolam
D. Ketamine bolus and propofol infusion
✅ Answer: B
Rationale: Frailty + cognition = spinal + sedation is safest.
2. Which of the following most increases the risk of postoperative delirium in the elderly?
A. Morphine infusion
B. Poorly controlled pain
C. Urinary catheter
D. All of the above
✅ Answer: D
Rationale: Pain, opioids, and catheters are all modifiable delirium risks.
3. An 80-year-old with CKD Stage 4 receives 5 mg IV morphine post-op. Hours later, he is confused and breathing shallowly. What is the likely cause?
A. Normal aging
B. Hypoxia
C. Accumulation of active morphine metabolites
D. Benzodiazepine use
✅ Answer: C
Rationale: Morphine is renally cleared — avoid in renal dysfunction.
4. During induction, an elderly man develops sudden hypotension without tachycardia. This is likely due to:
A. Propofol overdose
B. Baroreflex failure
C. Sepsis
D. Intravascular dehydration
✅ Answer: B
Rationale: Elderly have blunted baroreceptor responses — hypotension may not be compensated by HR rise.
5. Which agent is safest for sedation in a delirium-prone elderly patient?
A. Midazolam
B. Haloperidol
C. Dexmedetomidine
D. Diazepam
✅ Answer: C
Rationale: Dexmedetomidine provides sedation with less cognitive suppression.
6. You are performing spinal anesthesia for a 90-year-old woman with scoliosis. Which technique is most suitable?
A. Standard 3 mL of 0.5% bupivacaine
B. 5 mg bupivacaine with fentanyl + midazolam
C. Low-dose spinal (6 mg) + dexmedetomidine infusion
D. General anesthesia is always safer
✅ Answer: C
Rationale: Low-dose spinal + cautious sedation is best in scoliosis + age.
7. What is the most reliable early sign of postoperative deterioration in a frail elderly patient?
A. Bradycardia
B. Sudden drop in BP
C. Acute change in behavior or cognition
D. Fever
✅ Answer: C
Rationale: Delirium or confusion often precedes physical deterioration.
8. Which of the following is contraindicated in elderly patients with cognitive impairment?
A. Haloperidol
B. Midazolam
C. Dexmedetomidine
D. Fentanyl
✅ Answer: B
Rationale: Benzodiazepines increase risk of delirium and prolonged sedation.
9. You are planning a spinal block for an elderly patient with eGFR <30. Which opioid additive is safest?
A. Morphine
B. Tramadol
C. Fentanyl
D. Hydromorphone
✅ Answer: C
Rationale: Fentanyl is short-acting and metabolized hepatically.
10. A patient on warfarin with INR 2.8 presents for femoral hernia repair under spinal. What’s your next step?
A. Proceed with spinal
B. Reverse INR with Vitamin K
C. Switch to general anesthesia
D. Delay surgery
✅ Answer: B
Rationale: INR >1.4 is a contraindication to neuraxial anesthesia.
11. What is the age-adjusted MAC of sevoflurane in an 80-year-old?
A. 2.0
B. 1.0
C. 0.9
D. 0.6
✅ Answer: D
Rationale: MAC decreases ~6% per decade — lower doses needed.
12. Which of the following is not a red flag for perioperative complications in geriatrics?
A. Hearing loss
B. Poor nutrition
C. Polypharmacy
D. Age >65 alone
✅ Answer: D
Rationale: Age alone isn’t predictive without functional/clinical context.
13. What is the safest induction sequence for an elderly patient with heart failure and frailty?
A. Etomidate + fentanyl
B. Propofol 2 mg/kg + midazolam
C. Ketamine + midazolam
D. Thiopentone + suxamethonium
✅ Answer: A
Rationale: Etomidate maintains hemodynamics; avoid cardiac depressants.
14. Which is not a component of the Clinical Frailty Scale (CFS)?
A. Physical activity
B. Nutrition
C. Mobility
D. Gait speed
✅ Answer: D
Rationale: Gait speed is part of other scales, not CFS directly.
15. Which of the following is a recommended postoperative strategy to prevent POCD?
A. Keep patient sedated longer
B. Avoid pain medications
C. Early mobilization and orientation
D. Use high-dose dexmedetomidine
✅ Answer: C
Rationale: Early ambulation and reorientation reduce cognitive decline.
1️⃣1️⃣ Summary Tables & Pocket Reference Pages
📋 A. Clinical Frailty Scale (CFS) – 9-Point Summary
| CFS Score | Functional Description | Clinical Meaning |
|---|---|---|
| 1 | Very Fit | Robust, active, independent |
| 2 | Well | No active disease, slower |
| 3 | Managing Well | Medical problems well controlled |
| 4 | Vulnerable | Symptoms limit activities |
| 5 | Mildly Frail | Needs help with heavy tasks |
| 6 | Moderately Frail | Needs help with ADLs |
| 7 | Severely Frail | Dependent for personal care |
| 8 | Very Severely Frail | Fully dependent, nearing end of life |
| 9 | Terminally Ill | Life expectancy <6 months |
🧠 Clinical Tip: CFS ≥5 requires tailored anesthesia plans — avoid deep GA.
💊 B. Age-Adjusted MAC of Common Volatile Agents
| Age (Years) | Sevoflurane MAC | Isoflurane MAC | Desflurane MAC |
|---|---|---|---|
| 40 | 2.0 | 1.2 | 6.0 |
| 60 | 1.6 | 1.0 | 5.2 |
| 80 | 1.3 | 0.9 | 4.3 |
📌 Reminder: Always reduce volatile agent dose by ~6% per decade after age 40.
🧠 C. Safe Drug Use Quick Reference – Elderly Anesthesia
| Drug Class | Preferred Options | Cautions / Avoid |
|---|---|---|
| Induction Agents | Etomidate, low-dose Propofol | Avoid thiopental |
| Opioids | Fentanyl, Remifentanil | Avoid morphine, pethidine |
| Muscle Relaxants | Cisatracurium, Atracurium | Avoid pancuronium, vecuronium in CKD |
| Sedatives | Dexmedetomidine (slow), low ketamine | Avoid midazolam, diazepam |
| Reversal Agents | Sugammadex, Neostigmine/Glyco | Monitor TOF, avoid incomplete reversal |
📈 D. Geriatric Anesthesia Risk Flags – Memory Cue: “FRAIL AGE”
F – Frailty (CFS ≥5)
R – Renal dysfunction
A – Albumin low (<3.0 g/dL)
I – INR >1.5 or on anticoagulants
L – Low body weight / nutrition
A – Anemia (Hb <10)
G – Gait speed <0.8 m/s
E – Existing cognitive impairment
🔺 ≥3 factors = high-risk geriatric anesthetic candidate.
🚨 E. Emergency Post-op Delirium Protocol (Non-Pharma First)
| Step | Action |
|---|---|
| 1️⃣ | Orient – time, place, purpose |
| 2️⃣ | Remove – unnecessary lines/tubes |
| 3️⃣ | Ensure – glasses, hearing aids |
| 4️⃣ | Mobilize – as early as feasible |
| 5️⃣ | Family – allow presence if safe |
🛑 If pharmacologic needed:
Haloperidol 0.5–1 mg IV q8h max
Dexmedetomidine infusion (monitor HR closely)
🔟 Final Words
🧠 Judgment in Frailty
💉 Humility in Dosing
❤️ Dignity in the Elderly
Anesthesia in the elderly is not just a science of adjusted doses —
It is the art of recognizing fragility masked by silence, and responding with structure, vigilance, and grace.
Whether you’re in a fully equipped center with depth monitors and infusion pumps —
Or in a remote OR using spinal kits from the previous decade —
The risks are the same: delirium, decompensation, and delay.
But so are the principles:
🔷 You’ve now mastered:
🔹 The physiology of aging and organ vulnerability
🔹 The use of frailty scales to individualize plans
🔹 Tailored techniques for safety, recovery, and dignity
🔹 Postoperative vigilance to prevent cognitive collapse
This guide is your reference when facing geriatric patients in every setting —
From city hospitals to candlelit clinics running on courage and clinical instinct.
Stay structured. Stay vigilant. Act wisely. 🧠
📌 Prepared for Dr. Amir Fadhel — Specialist in Anesthesiology and Critical Care
📅 Created: 11/06/2025
📅 Last Updated: 11/06/2025
🔗 Explore the Mastery Series: https://justpaste.it/jkd89