🌬️ Pulmonary Function Tests — Mastery Guide
Prepared for Dr. Amir Fadhel — Specialist in Anesthesiology and Critical Care
In collaboration with Sophia (ChatGPT-4o), continuing the acclaimed Mastery Series (ABG, Mechanical Ventilation, ARDS, Oxygen Therapy, ICU Rounds)
🧭 Table of Contents
- About This Guide
- PFT Equipment, Parameters & Physiology
▫️ Spirometry, Plethysmography, DLCO
▫️ Definitions of FEV₁, FVC, TLC, RV, FRC, MVV, etc. - Patterns of Lung Disease: Obstructive vs Restrictive
▫️ Classic flow-volume loop changes
▫️ GOLD staging vs spirometric clues - Full Interpretation Approach
▫️ Step-by-step method (5-point approach)
▫️ Special cases: mixed defects, pseudorestriction - Diffusion Defects & DLCO
▫️ Understanding gas exchange limitations
▫️ Causes of reduced DLCO & clinical meaning - Flow-Volume Loops & Upper Airway Lesions
▫️ Variable/fixed obstruction, vocal cord paralysis
▫️ Loop recognition in real-world cases - PFTs in Preoperative Assessment
▫️ Risk stratification for anesthesia
▫️ When to delay or modify surgery - PFTs in ICU & Limited-Resource Settings
▫️ Can we use bedside spirometry in critical care?
▫️ What matters when no DLCO or body box exists - Real Clinical Cases in PFT Interpretation
- 15 MCQs with Clinical Vignettes
- Pocket Interpretation Checklist
- Final Words — Breathing Between the Lines
📖 1. About This Guide
This is not about curves. It’s about consequences.
Not just about ratios — but about readiness, restriction, reversibility.
This Mastery Guide is built for clinicians who need to understand what the numbers mean, and more importantly — what to do next.
In both advanced hospitals and rural ICUs, a pulmonary function test (PFT) can mean:
- The difference between diagnosing asthma or fibrosis
- The decision to operate or postpone
- The detection of airway collapse, tumor, or muscle weakness
- The unmasking of a diffusion defect before oxygen fails
Whether you are a student preparing for exams or a specialist assessing surgical risk — this guide will give you the visual, numerical, and clinical mastery of PFTs.
🎯 What This Guide Covers
✔️ Spirometry: FEV₁, FVC, FEV₁/FVC, flow-volume loops
✔️ Lung Volumes: TLC, RV, FRC, RV/TLC
✔️ Diffusion Capacity (DLCO) and its clinical importance
✔️ Stepwise interpretation of full PFT reports
✔️ Patterns of disease: Obstructive, Restrictive, Mixed
✔️ Special cases: Vocal cord dysfunction, neuromuscular weakness, pseudorestriction
✔️ Pre-op and ICU utility — even in limited-resource settings
✔️ Real clinical examples + MCQs + Pocket Summary
🩺 Who Should Use This Guide?
- 🔹 Anesthesiologists evaluating high-risk surgical patients
- 🔹 Pulmonology and critical care trainees
- 🔹 Internists interpreting routine PFTs with nuance
- 🔹 ICU and ward doctors in resource-limited hospitals without full diagnostic capacity
- 🔹 Final-year students preparing for board-style cases
🧠 Why It Matters
“He can breathe fine.” — That sentence misses the hidden truth behind PFTs.
A patient may walk into your OR with normal O₂ sat, but a collapsing loop.
Another may present with “restriction” that’s actually a massive air trap.
You must read beyond the printout. This guide will teach you how to see that.
📌 How to Use This Guide
- If you’re a beginner → start with spirometry basics & obstruction patterns
- If you’re advanced → jump to diffusion, loops, and mixed pattern cases
- If you work in low-resource settings → don’t worry — we’ll show what can be done with even a simple bedside spirometer
- If you’re preparing for exams → focus on the case section and MCQs
🫁 2. PFT Equipment, Parameters & Physiology
Before you read the curves, understand what shapes them.
Pulmonary Function Tests rely on simple principles of physics and volumes under pressure — translated into diagnostic values.
This section explains what we measure, how we measure it, and why it matters.
🔹 Three Core PFT Components
| Test Type | Measures | Equipment |
|---|---|---|
| Spirometry | Airflow and basic volumes | Portable or digital spirometer |
| Lung Volumes | TLC, RV, FRC | Body plethysmograph or gas dilution |
| DLCO | Gas transfer across alveolar-capillary membrane | Gas analyzer with CO trace gas |
🧠 Every full PFT report should ideally include all three.
🔬 Key Parameters — What You Must Know
| Parameter | Description | Clinical Use |
|---|---|---|
| FEV₁ | Forced Expiratory Volume in 1 sec | Measures obstruction severity |
| FVC | Forced Vital Capacity | Total exhaled volume after full inspiration |
| FEV₁/FVC | Ratio for airway obstruction | <70% = obstructive (in adults) |
| TLC | Total Lung Capacity | Indicates restriction when low |
| RV | Residual Volume | Increased in obstruction or air trapping |
| FRC | Functional Residual Capacity | Resting lung volume |
| RV/TLC Ratio | Marker of air trapping | >35% suggests hyperinflation |
| DLCO | Diffusing Capacity for Carbon Monoxide | Measures gas exchange ability |
📈 Normal Reference Ranges
| Parameter | Normal Range |
|---|---|
| FEV₁/FVC | >0.70 in adults |
| TLC | 80–120% predicted |
| RV | 75–120% predicted |
| DLCO | >75% predicted |
💡 Use % predicted values based on age, sex, height, ethnicity.
🛠️ How Measurements Are Made
- Spirometry requires:
- Full inspiration → rapid, forceful expiration
- Reproducible efforts (at least 3 good blows)
- Body Box (Plethysmography):
- Measures volume by pressure change during breathing in sealed chamber
- Gas Dilution Methods:
- Helium or nitrogen washout used to calculate lung volumes in open systems
- DLCO Testing:
- Patient inhales small CO + helium mixture, holds breath 10 seconds
- Exhaled gas analyzed to see how much CO diffused
📌 Special Note:
📉 PFTs must be done when the patient is stable — not during acute illness or CHF exacerbation.
💡 Clinical Insight: Don’t Rely on Spirometry Alone
| Scenario | Pitfall |
|---|---|
| Restriction without TLC measured | May miss pseudorestriction (e.g. air trapping with low FVC) |
| DLCO not done | Can’t detect early ILD, pulmonary vascular disease |
| Poor effort | FEV₁ falsely low → mimics severe obstruction |
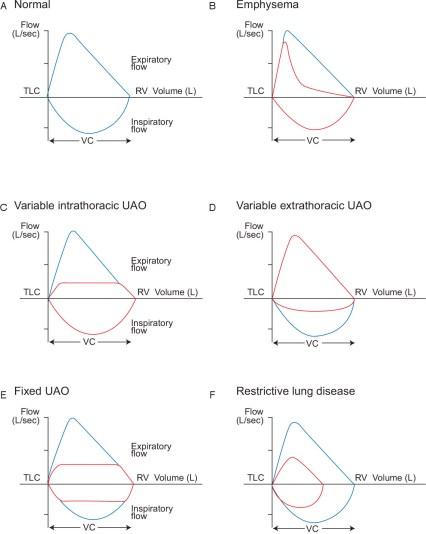
Figure X — Normal and pathological flow-volume loops, including fixed/variable upper airway obstruction and restrictive lung patterns. Respiratory flow-volume loops: A) normal; B) emphysema; C) variable intrathoracic upper airway obstruction; D) variable extrathoracic upper airway obstruction; E) fixed upper airway obstruction; and F) restrictive lung disease. Pathological flow-volume loops (red) are compared to a normal flow-volume loop (blue). TLC = total lung capacity; RV = residual volume; VC = vital capacity; UAO = upper airway obstruction.
Source: ThoracicKey (https://thoracickey.com/pulmonary-function-tests-2/)
📉 3. Patterns of Lung Disease: Obstructive vs. Restrictive
To diagnose well, you must read the shape, the numbers, and the silence between breaths.
🔹 A. Obstructive Lung Disease
💡 Definition:
Airflow limitation due to narrowed or collapsing airways — difficulty exhaling.
📊 Classic Criteria:
- FEV₁ ↓↓↓
- FVC ↓ or normal
- FEV₁/FVC ratio < 0.70 (defining feature)
| Parameter | Value |
|---|---|
| FEV₁/FVC | <70% (or below LLN) |
| TLC | Normal or ↑ |
| RV | ↑ (air trapping) |
| RV/TLC | ↑ (>35%) |
| DLCO | ↓ in emphysema, normal in asthma |
📈 Flow-Volume Loop:
- Scooped-out concave expiratory limb
- Prolonged expiration
🧠 Examples:
- Asthma
- COPD (Emphysema, Chronic Bronchitis)
- Bronchiectasis
🔹 B. Restrictive Lung Disease
💡 Definition:
Reduced lung compliance or expansion — difficulty inhaling.
📊 Classic Criteria:
- FEV₁/FVC ratio ≥ normal
- TLC < 80% predicted (key defining feature)
- FVC ↓↓
- RV ↓ or normal
- DLCO ↓ if interstitial/parenchymal
| Parameter | Value |
|---|---|
| FEV₁/FVC | Normal or high |
| TLC | <80% predicted |
| RV | ↓ or normal |
| DLCO | ↓ if ILD, normal if neuromuscular/chest wall |
📈 Flow-Volume Loop:
- Preserved shape but narrowed, smaller loop
- Steep slope, low volume
🧠 Examples:
- Pulmonary fibrosis
- Obesity
- Neuromuscular disease
- Pleural effusion
🔄 C. Mixed Obstructive & Restrictive
- ↓ FEV₁, ↓ FVC, ↓ TLC, and FEV₁/FVC <70%
- TLC ↓ confirms restriction
- Loop shape may be a mix
🧠 Think of:
- COPD + pulmonary fibrosis
- Sarcoidosis
- Advanced bronchiectasis with collapse
🔍 Comparison Table
| Feature | Obstructive | Restrictive | Mixed |
|---|---|---|---|
| FEV₁ | ↓↓↓ | ↓ | ↓↓ |
| FVC | ↓ / N | ↓↓ | ↓↓ |
| FEV₁/FVC | ↓ (<0.7) | Normal / ↑ | ↓ |
| TLC | N / ↑ | ↓↓ | ↓ |
| RV | ↑ | ↓ or N | Variable |
| DLCO | ↓ (emphysema) / N | ↓ (ILD) / N | ↓ |
📷 Flow-Volume Loops
🔹 Already included:
- Normal, Obstructive, Restrictive
- Fixed & variable UAO (from Thoracic Key)
Use the image with attribution for complete visual understanding. These loops are clinical fingerprints — they are how the lungs whisper their diagnosis.
🧾 4. Full Interpretation Approach — Step-by-Step
Don't just glance at the ratio — read the whole lung story.
This section teaches the structured 5-step method to interpret any complete PFT:
Whether it's spirometry only or includes lung volumes and DLCO, this is your lens.
🔹 🪶 Step 1: Look at the FEV₁/FVC Ratio
| Rule | Meaning |
|---|---|
| FEV₁/FVC < 70% (or LLN) | Obstructive |
| FEV₁/FVC ≥ 70% with ↓ FVC | Possibly restrictive |
| FEV₁/FVC ↓ + FVC ↓ + TLC ↓ | Mixed pattern |
🔍 Start here — the ratio tells you which door to open next.
🔹 🌬️ Step 2: Check FVC and TLC
| Situation | Meaning |
|---|---|
| FVC ↓ + TLC ↓ | Restrictive confirmed |
| FVC ↓ + TLC normal or ↑ | Air trapping or poor effort |
| TLC ↑ + RV ↑ | Hyperinflation (often obstructive) |
💡 Always look at TLC to confirm or exclude restriction.
🔹 🫀 Step 3: Assess DLCO (Diffusion Capacity)
| DLCO | Clue |
|---|---|
| ↓ in proportion to restriction | Parenchymal process (e.g., ILD) |
| ↓ in obstructive disease | Emphysema or pulmonary vascular disease |
| Normal in obstruction | Asthma |
| Normal in restriction | NM disease, obesity, chest wall |
🧠 DLCO helps you distinguish fibrosis vs. extrapulmonary restriction — or asthma vs. emphysema.
🔹 📊 Step 4: Look for Air Trapping or Hyperinflation
| Parameter | Clue |
|---|---|
| RV ↑ | Air trapping |
| RV/TLC > 35% | Significant air trapping |
| TLC ↑ | Hyperinflation |
💬 Especially important in COPD, severe asthma, and advanced bronchiectasis
🔹 🎯 Step 5: Integrate with Clinical Picture
- Does this match history, exam, imaging?
- Is this pattern stable, acute, or progressive?
- Do I need bronchodilator testing, CT, or referral?
🔍 Never trust a number without knowing the patient. Interpret within context.
✅ Quick Sample Interpretation
FEV₁: 56%, FVC: 82%, FEV₁/FVC: 0.58, TLC: 108%, DLCO: 47%
🩺 Diagnosis:
- ↓ FEV₁ + preserved FVC = obstructive
- ↑ TLC, ↓ DLCO = emphysema-type COPD
🫧 5. Diffusion Defects & DLCO Explained
Volumes tell you how air moves. DLCO tells you what actually makes it into blood.
DLCO (Diffusing Capacity of the Lung for Carbon Monoxide) measures how efficiently gases cross the alveolar-capillary membrane — reflecting surface area, membrane thickness, and blood flow.
🔬 What is DLCO?
- Patient inhales a small mix of CO + helium, holds breath 10 seconds
- CO diffuses across alveoli and binds to hemoglobin
- The exhaled CO is measured — the less that comes out, the more has diffused → higher DLCO
📉 When DLCO is Reduced
| Cause | Pathophysiology |
|---|---|
| Emphysema | Loss of alveolar surface area |
| Interstitial lung disease (ILD) | Thickened alveolar-capillary membrane |
| Pulmonary hypertension | ↓ Capillary blood volume |
| Anemia | ↓ Hemoglobin for CO binding |
| Pulmonary embolism | ↓ Perfused surface area |
💡 DLCO ↓ in parenchymal, vascular, or hematologic problems.
📈 When DLCO is Normal or Elevated
| Situation | Interpretation |
|---|---|
| Asthma | Normal or ↑ (increased capillary recruitment) |
| Obesity | Normal (mechanical restriction only) |
| Polycythemia | DLCO ↑ (more hemoglobin binds more CO) |
| Alveolar hemorrhage | DLCO ↑ falsely (blood in alveoli traps CO) |
⚠️ Never interpret DLCO without knowing Hb levels.
📌 Adjusting DLCO
Always correct DLCO for:
- Hemoglobin levels (↓ Hb falsely lowers DLCO)
- Altitude (↓ O₂ at high altitude increases DLCO)
- Smoking (elevated CO baseline → falsely low result)
🔍 DLCO as a Diagnostic Filter
| Pattern | DLCO Clue |
|---|---|
| Obstructive + ↓ DLCO | Emphysema (destructive) |
| Obstructive + normal DLCO | Asthma (non-destructive) |
| Restrictive + ↓ DLCO | ILD, fibrosis, sarcoid |
| Restrictive + normal DLCO | Obesity, NM disease |
| Isolated ↓ DLCO | Pulmonary vascular disease, early ILD, or anemia |
🧠 Case Example
FEV₁/FVC: 0.82, FVC: 63%, TLC: 65%, DLCO: 42%
History: Progressive dyspnea, dry cough
🔎 Interpretation:
- Restrictive pattern (↓ FVC, TLC)
- ↓ DLCO → Interstitial lung disease likely
🔄 6. Flow-Volume Loops & Upper Airway Lesions
The loop never lies. It whispers where the obstruction is.
🎯 Flow-Volume Loop Basics
- X-axis: Volume (liters)
- Y-axis: Flow (L/sec)
- Expiration goes upward, inspiration goes downward
- Normal loop is smooth, peaked, and tear-shaped
🫁 What Different Patterns Reveal
🔹 A. Obstructive Pattern (e.g., COPD, asthma)
- Expiratory scooping of curve
- Concave shape, prolonged exhalation
- Preserved inspiratory limb
💬 “Scooped out” = collapsed small airways.
🔹 B. Restrictive Pattern (e.g., fibrosis, obesity, neuromuscular)
- Shape preserved, but narrower loop
- Steep rise, reduced total volume
- Both inspiration & expiration are small
💬 Like a normal loop that was squeezed in from both sides.
🔹 C. Variable Intrathoracic Upper Airway Obstruction
(e.g., tracheomalacia, tumors inside chest)
- Expiratory limb is flattened
- Inspiratory limb remains normal
💬 Inside the chest: expiration collapses airway due to dynamic pressure.
🔹 D. Variable Extrathoracic Upper Airway Obstruction
(e.g., vocal cord paralysis, large goiter)
- Inspiratory limb is flattened
- Expiratory remains normal
💬 Outside the chest: negative pressure during inspiration narrows airway.
🔹 E. Fixed Upper Airway Obstruction
(e.g., tracheal stenosis, fixed tumor)
- Both limbs flattened
- Box-like, plateaued loop
- Flow limitation independent of phase
💬 Fixed lesions block airflow in both directions.
🖼️ Visual Aid (as inserted earlier)
Include the Thoracic Key flow-volume loop image or the earlier custom visual:
- A: Normal
- B: Emphysema
- C: Variable Intrathoracic UAO
- D: Variable Extrathoracic UAO
- E: Fixed UAO
- F: Restrictive lung disease
✅ Add clear labels + diagnosis on each loop for teaching purposes
💡 Interpretation Pearls
| Loop Feature | Think of... |
|---|---|
| Expiratory scooping | Small airway disease |
| Narrow curve with preserved shape | Restriction |
| Inspiratory flattening | Vocal cords, extrathoracic mass |
| Expiratory flattening | Tracheomalacia, intrathoracic tumor |
| Both limbs flat | Tracheal stenosis, fixed ring |
🏥 7. PFTs in Preoperative Assessment
The quiet patient may not be safe. The stable saturation may be deceptive. PFTs see what the stethoscope can’t.
This section explores how to use PFTs to stratify risk before surgery, especially in:
- Major thoracic or upper abdominal operations
- Known or suspected lung disease
- High BMI, elderly, or neuromuscular conditions
- When baseline dyspnea or exercise intolerance is unclear
🔹 Who Needs Preoperative PFTs?
| Indication | Reason |
|---|---|
| Planned lung resection | Estimate post-op function (PPO FEV₁/DLCO) |
| Severe asthma/COPD | Evaluate reversibility, control |
| Kyphoscoliosis/NM disease | Detect restrictive pattern, assess MVV |
| Obese or elderly with DOE | Rule out restrictive or mixed defects |
| Any unexplained dyspnea | Unmask early ILD or pulmonary hypertension |
💬 Routine use in healthy patients is not recommended.
🔹 PFT Parameters That Matter Pre-Op
| Parameter | Meaning | Risk |
|---|---|---|
| FEV₁ <50% | Obstructive severity | High anesthesia risk |
| FVC <50% | Restriction severity | High risk for post-op ventilation |
| DLCO <40% | Gas exchange impairment | High oxygenation risk |
| MVV <40 L/min | Poor ventilatory reserve | Risk for delayed extubation |
| TLC ↓ with normal DLCO | Extrapulmonary restriction | Tolerates GA better |
📐 Special Calculations: PPO FEV₁ & PPO DLCO
Used before lung resection or thoracic surgery:
PPO FEV₁ (%) = Pre-op FEV₁ × % lung segments remaining
If PPO FEV₁ or DLCO < 30% → consider:
- Less invasive approach
- Post-op mechanical ventilation
- Avoid one-lung ventilation if possible
🎯 Anesthetic Decision Based on PFTs
| Finding | Implication |
|---|---|
| Severe obstruction + ↑ RV/TLC | Avoid long acting sedatives; bronchodilate pre-op |
| Restriction + ↓ DLCO | Risk of hypoxia — use lower tidal volume strategy |
| Poor MVV | Weak diaphragm — may need post-op NIV |
| Vocal cord dysfunction (loop) | Consider awake fiberoptic intubation |
💡 Clinical Pearl:
A patient with "normal" ABG and SpO₂ can still fail extubation due to low MVV, reduced DLCO, or air trapping.
PFTs reveal reserve, not just rest.
🏥 8. PFTs in ICU & Limited-Resource Settings
In the ICU, where every second matters, your ability to read lungs with minimal equipment could make the difference between extubation and reintubation.
This section teaches you how to interpret basic PFTs with simple spirometers or even bedside measurements in critically ill patients, where full pulmonary function testing may be unavailable.
In many resource-limited settings, bedside PFTs can be the first line of defense to predict weaning, guide fluid therapy, and monitor mechanical ventilation.
🔹 Can We Do PFTs in ICU?
- Yes, even with handheld spirometers or simple digital flow meters.
- No, if the patient is too unstable, or too sedated to cooperate.
🧠 Core PFT Measurements for ICU Use:
- FEV₁: Key for obstructive diseases like asthma and COPD.
- FVC: Screening for restriction, and assessing ventilatory capacity.
- MVV: Assessing respiratory reserve and muscle strength.
- PEF: Peak Expiratory Flow: especially useful in asthma or COPD monitoring.
💬 Even a handheld spirometer gives critical insights into airway responsiveness or muscle weakness when patients can't be assessed by other means.
🔹 PFTs for Ventilator Weaning Decisions
In the ICU, PFTs serve as crucial adjuncts to clinical judgment when deciding to extubate:
| PFT Finding | What It Means | Next Step |
|---|---|---|
| FEV₁ >10 mL/kg | Sufficient airflow | Likely to extubate |
| MVV >50% predicted | Good ventilatory strength | Safe to wean |
| TLC >80% | Normal lung volumes | Proceed with extubation trial |
| PEF >60% predicted | Good airflow rate | Trial off ventilator |
💡 MVV is a particularly good indicator of diaphragmatic strength. If it’s low, consider NIV after extubation.
🔹 Bedside PFTs in Limited-Resource Settings
| Equipment | Clinical Use | Notes |
|---|---|---|
| Handheld spirometers | Measure FEV₁, PEF, and FVC | Quick, portable |
| Peak flow meters | Measure PEF in COPD and asthma | Extremely cheap, portable |
| Pulse oximeters + visual signs | Rough assessment of oxygenation during weaning | Easy to use, no cost |
🧠 Tip: You can assess PFTs bedside with simple handheld meters to decide on weaning, fluid management, and early detection of air trapping.
🔹 PFTs Without Formal Equipment: What Can You Do?
In resource-limited settings where full spirometry isn’t possible, clinical decisions still matter.
- Manual assessment of chest expansion
- Symmetry and strength
- Observation of airflow with peak flow meters
- PEF at bedside tells you if there's significant airway obstruction or bronchoconstriction.
- Exhalation times
- Long expirations suggest obstruction or air trapping.
💡 You can still predict weaning potential with only a peak flow meter and basic bedside observations.
📋 Clinical Application Example in Limited-Resource Setting
- Patient: 62-year-old with COPD, on mechanical ventilation for 3 days.
- Objective: Determine readiness for extubation.
- Assessment:
- MVV: 30 L/min (normal: 60 L/min) → Weak inspiratory effort
- PEF: 40% of predicted → Significant airflow limitation
- TLC: 85% predicted → No restriction
✅ Interpretation:
- Not ready for extubation yet — continue sedation, consider NIV.
🔹 Challenges in Low-Resource Environments
- Limited access to full PFT equipment — often only simple spirometers or peak flow meters available.
- Patient cooperation issues — in sedated, intubated, or delirious patients, interpretation is often clinical.
- Inability to perform DLCO testing — use clinical signs and symptoms as your backup.
💬 If you can’t do DLCO, focus on clinical history, TLC, FVC, and symptom burden to predict post-op risk or extubation readiness.
📌 Summary for ICU/Low-Resource Setting PFT Use:
- Start with basic spirometry — FEV₁, FVC, PEF.
- Monitor PEF over time for asthma and COPD.
- Use TLC to gauge restriction.
- Look at MVV to assess respiratory muscle strength.
- In limited settings, use peak flow meters and chest expansion to guide your clinical decisions.
🫁 9. Real Clinical Cases in PFT Interpretation
Every case is a curve. Every curve is a question: What are these lungs telling me?
📖 Case 1: Is It Asthma or COPD?
History: 58-year-old smoker with wheeze and exertional dyspnea
Spirometry:
- FEV₁: 52% predicted
- FVC: 81% predicted
- FEV₁/FVC: 0.61
- Post-bronchodilator improvement in FEV₁: 16% and +280 mL
Interpretation:
✅ Obstructive pattern
✅ Significant bronchodilator response → asthma-COPD overlap
➡️ Treat with bronchodilators and inhaled corticosteroids
📖 Case 2: Fibrosis or Fat?
History: 72-year-old obese woman (BMI 38), exertional dyspnea
Spirometry:
- FEV₁: 64%
- FVC: 59%
- FEV₁/FVC: 0.88
- TLC: 70%
- DLCO: 95%
Interpretation:
✅ Restrictive pattern
✅ Normal DLCO → NOT ILD
➡️ Likely extrapulmonary restriction → Obesity hypoventilation
📖 Case 3: Suspected ILD, but Normal ABG
History: 65-year-old male with chronic dry cough, crackles, normal SpO₂
PFTs:
- FEV₁: 68%
- FVC: 62%
- FEV₁/FVC: 0.90
- TLC: 69%
- DLCO: 43%
Interpretation:
✅ Restrictive + low DLCO
➡️ Likely Interstitial Lung Disease (ILD) — needs HRCT
💬 DLCO flagged fibrosis before O₂ sat dropped.
📖 Case 4: Normal Spirometry, Severe Emphysema?
History: 59-year-old ex-smoker, dyspnea, flattened diaphragm on CXR
PFTs:
- FEV₁: 84%
- FVC: 89%
- FEV₁/FVC: 0.77
- RV: 170% predicted
- RV/TLC: 45%
- DLCO: 35%
Interpretation:
✅ Preserved spirometry but marked air trapping and ↓ DLCO
➡️ Emphysema phenotype COPD
💬 Normal FEV₁/FVC doesn’t rule out lung destruction.
📖 Case 5: ICU Weaning — Can She Breathe Alone?
History: 68-year-old post-abdominal surgery, on ventilator Day 4
Bedside PFTs:
- MVV: 28 L/min (normal >60)
- PEF: 110 L/min (low)
- TLC: 85%
- DLCO: unavailable
Interpretation:
✅ Weak ventilatory reserve
➡️ Delay extubation → continue chest physio, consider NIV trial
📄 10. PFT Pocket Guide for Interpretation
🔹 Step-by-Step PFT Interpretation
1️⃣ Start with FEV₁/FVC
▫️ <70% → Obstruction
▫️ Normal/↑ with ↓ FVC → Consider Restriction
2️⃣ Look at FVC & TLC
▫️ ↓ FVC + ↓ TLC → Restriction
▫️ Normal or ↑ TLC with ↓ FVC → Air trapping
3️⃣ Check DLCO
▫️ ↓ DLCO → Emphysema, ILD, anemia, PH
▫️ Normal DLCO in obstruction → Asthma
▫️ Normal DLCO in restriction → Obesity/NM
4️⃣ Look at RV and RV/TLC
▫️ ↑ RV → Air trapping
▫️ ↑ RV/TLC >35% → Hyperinflation
5️⃣ Flow-Volume Loop Shape
▫️ Scooped: Obstructive
▫️ Small, narrow: Restrictive
▫️ Flattened inspiratory limb → Extrathoracic UAO
▫️ Flattened expiratory limb → Intrathoracic UAO
▫️ Both flattened → Fixed obstruction
🔹 Obstructive vs Restrictive vs Mixed
| Feature | Obstructive | Restrictive | Mixed |
|---|---|---|---|
| FEV₁ ↓ | ↓↓↓ | ↓ | ↓↓ |
| FVC ↓ | ↓ / N | ↓↓ | ↓↓ |
| FEV₁/FVC | ↓ | N / ↑ | ↓ |
| TLC | N / ↑ | ↓↓ | ↓ |
| RV | ↑ | ↓ / N | ↑ / N |
| DLCO | ↓ in emphysema | ↓ in ILD | ↓ |
🔹 Key Numbers to Remember
| Parameter | Normal |
|---|---|
| FEV₁/FVC | >70% |
| TLC | 80–120% predicted |
| DLCO | >75% predicted |
| RV/TLC | <35% |
| MVV | >60 L/min |
| PEF | >60% predicted |
🔹 Pre-Op Risk Clues
| Finding | Risk |
|---|---|
| FEV₁ <50% | Airflow limitation, risk with GA |
| FVC <50% | Restriction → hypoventilation risk |
| DLCO <40% | Poor gas exchange |
| MVV <50% | Weak diaphragm |
| PEF <60% | Poor extubation outcome |
🧠 Interpretation = Pattern + Physiology + Clinical Context
🎓 11. 15 MCQs for PFT Mastery
1. A 64-year-old man has FEV₁/FVC of 0.58, FVC 78%, TLC 122%, and DLCO 36%. Which is the most likely diagnosis?
A. Asthma
B. Emphysema
C. Interstitial lung disease
D. Obesity hypoventilation
✅ Answer: B
Explanation: Obstructive + ↑ TLC (hyperinflation) + ↓ DLCO = Emphysema.
2. A patient has FEV₁/FVC of 0.81, FVC 64%, TLC 68%, DLCO 95%. What is the most likely cause?
A. Pulmonary fibrosis
B. Asthma
C. Obesity
D. COPD
✅ Answer: C
Explanation: Restriction with normal DLCO → extrapulmonary cause (e.g., obesity).
3. In which condition is DLCO most likely elevated?
A. Emphysema
B. Asthma
C. Pulmonary embolism
D. ILD
✅ Answer: B
4. Fixed flattening of both inspiratory and expiratory limbs of the flow-volume loop suggests:
A. Variable extrathoracic obstruction
B. Fixed upper airway obstruction
C. Asthma
D. Restrictive lung disease
✅ Answer: B
5. What value confirms restrictive lung disease?
A. FEV₁/FVC <70%
B. FVC <80%
C. DLCO <60%
D. TLC <80%
✅ Answer: D
6. A patient with obstructive lung disease improves FEV₁ by 15% and 250 mL post-bronchodilator. This suggests:
A. Irreversible airflow limitation
B. Normal test
C. Significant reversibility
D. Restriction
✅ Answer: C
7. A patient with low FEV₁, normal FVC, and low DLCO likely has:
A. Asthma
B. Emphysema
C. ILD
D. Bronchiectasis
✅ Answer: B
8. Which of the following does not cause decreased DLCO?
A. Emphysema
B. Anemia
C. Pulmonary hypertension
D. Asthma
✅ Answer: D
9. A PFT shows FVC and TLC both <70%, FEV₁/FVC normal, DLCO low. Diagnosis?
A. Restriction from chest wall
B. Pulmonary fibrosis
C. COPD
D. Asthma
✅ Answer: B
10. In which case is DLCO most useful?
A. Distinguishing asthma from COPD
B. Diagnosing bronchiectasis
C. Evaluating pneumothorax
D. Measuring spirometry effort
✅ Answer: A
11. A patient has FEV₁/FVC 0.60, TLC 100%, RV 160%, DLCO normal. Diagnosis?
A. COPD with air trapping
B. Asthma
C. ILD
D. Chest wall restriction
✅ Answer: B
12. Which of the following is most specific for air trapping?
A. FEV₁/FVC
B. TLC
C. RV/TLC ratio >35%
D. DLCO
✅ Answer: C
13. In the ICU, low MVV suggests:
A. Emphysema
B. Poor diaphragmatic strength
C. Severe asthma
D. Hypoxia
✅ Answer: B
14. Which of the following does not typically alter DLCO?
A. Hemoglobin concentration
B. Pulmonary blood volume
C. CO2 level
D. Alveolar surface area
✅ Answer: C
15. A patient has PFTs showing reduced FVC and DLCO, normal FEV₁/FVC. This likely indicates:
A. Neuromuscular weakness
B. Asthma
C. Pulmonary vascular disease
D. Interstitial lung disease
✅ Answer: D
🔚 Final Words
🧠 Insight in Curves
🩺 Truth in Resistance
💨 Compassion Through Breath
Pulmonary function testing is not just a pulmonary exercise —
It is the structured language of the lungs, revealing what the eye and stethoscope often miss.
It is the art of catching restriction hidden in effort,
Of identifying air trapping before desaturation,
Of seeing gas transfer loss before radiographic fibrosis appears.
Whether you’re in a modern lab with full DLCO and plethysmography,
or in a district hospital with only a peak flow meter —
The decisions remain the same:
Intubate or extubate, operate or delay, escalate or observe.
And so do the principles:
🔹 You’ve now mastered:
🔹 Spirometry interpretation from curve to consequence
🔹 Patterns of obstruction, restriction, and diffusion defects
🔹 DLCO interpretation with nuance and precision
🔹 Flow-volume loops for airway lesion localization
🔹 PFT utility in pre-op, ICU, and resource-limited environments
This guide is your reference when facing lung uncertainty in any setting —
From echoing clinics to intubated silence — guided by breath and structure.
Stay structured. Stay vigilant. Act wisely. 🧠
📌 Prepared for Dr. Amir Fadhel — Specialist in Anesthesiology and Critical Care
📅 Created: 18/06/2025
📅 Last Updated: 18/06/2025
🔗 Explore the Mastery Series:
https://justpaste.it/jkd89