🧸 Pediatric Anesthesia — Mastery Guide
Safe Practices, Smart Strategies, and Real-World Applications
📎 Prepared for Dr. Amir Fadhel — Specialist in Anesthesiology and Critical Care
In collaboration with Sophia (ChatGPT-4o) | Clinical Teaching & Mastery Series
Absolutely, Amir — here is the official “About This Guide” section for our Pediatric Anesthesia — Mastery Guide, formatted professionally and styled like our previous series entries:
📘 About This Guide
This guide is part of the Clinical Mastery Series that began with the acclaimed ABG Interpretation Journey, expanding into Shock, Mechanical Ventilation, ARDS, Sepsis, Electrolytes, and more.
Pediatric anesthesia is a uniquely demanding field requiring age-specific knowledge, meticulous dosing, and anticipation of rapid physiologic shifts. This guide was designed to:
- 🧠 Simplify core concepts in pediatric airway, pharmacology, and physiology
- ✍️ Organize the knowledge step-by-step for students, trainees, and practicing clinicians
- 🛡️ Prepare anesthetists for emergencies, red flags, and tricky syndromes
- 🌍 Bridge the gap between high-tech and limited-resource environments
- 🎓 Reinforce learning through MCQs and bedside-ready tips
Whether you’re preparing for pediatric cases in a tertiary center, a rural hospital, or a mission setting, this guide provides the clarity, structure, and confidence you need.
📖 Table of Contents
- Core Sections
1️⃣ Introduction to Pediatric Anesthesia
2️⃣ Preoperative Assessment: Age, Weight, Syndromes, Developmental Stage
3️⃣ Pediatric Airway & Equipment Sizing
▫️ Airway anatomy by age
▫️ ETT size and depth formulas
▫️ LMA, blades, mask, suction tips
4️⃣ Drug Dosing in Pediatrics: Tables & Clinical Calculators
▫️ Induction agents, opioids, relaxants, reversal
▫️ Resuscitation drugs (e.g., adrenaline 10 mcg/kg)
▫️ Amir’s preferred formula: (Age ÷ 4) + 4
5️⃣ Induction Techniques: Inhalational vs IV in Practice
▫️ Sevo vs Halothane
▫️ Ketamine for IV induction
▫️ Handling difficult venous access
6️⃣ Maintenance & Monitoring: Gases, TIVA, Depth, and Vitals
▫️ SpO₂, EtCO₂, NIRS, temperature
▫️ Age-based MAC values
▫️ IV fluids, glucose needs, thermoregulation
7️⃣ Emergence & Recovery: Laryngospasm, Agitation, Hypoxia
▫️ Deep vs awake extubation
▫️ Pain vs emergence delirium
▫️ Post-op oxygen & glucose monitoring
- ADVANCED & DIFFERENTIATING SECTIONS
8️⃣ Emergency Troubleshooting: What to Do When Things Go Wrong
📌 Flowcharts and checklist responses to:
▫️ Laryngospasm
▫️ Bradycardia
▫️ Post-intubation desaturation
▫️ IV access failure
▫️ Inhalational induction complications
9️⃣ Anesthesia for Common Pediatric Surgeries – Mini Playbooks
🛠️ Fast reference briefs for common OR cases:
▫️ Inguinal hernia
▫️ Circumcision
▫️ Tonsillectomy
▫️ Appendectomy
▫️ VP shunt & hydrocephalus
🔟 Perioperative Challenges in Pediatric Comorbidities
🎯 Disease-based planning, split into:
▫️ Cardiovascular (e.g., TOF, VSD, Eisenmenger)
▫️ Respiratory (e.g., URTI, LRTI, RSV)
▫️ Neurological & Syndromic (e.g., Down, CP, epilepsy)
▫️ GI, Renal, Metabolic (e.g., GERD, renal dysplasia, diabetes)
▫️ Plus: craniofacial anomalies, immunocompromised, post-COVID
1️⃣1️⃣ Parental Counseling & Preoperative Communication
▫️ Explaining anesthesia simply
▫️ Managing separation anxiety
▫️ Questions parents ask
▫️ Cultural considerations in Arab & Iraqi settings
1️⃣2️⃣ Pediatric Analgesia & Regional Blocks
▫️ Multimodal strategy
▫️ Caudal, penile block, TAP block
▫️ Opioid-sparing tips in tonsillectomy, hernia repair
1️⃣3️⃣ Low-Resource Toolbox
🛠️ Adapting in district hospitals or rural centers:
▫️ No Sevo? Use Halothane safely
▫️ Modify adult circuits and masks
▫️ Warm babies without Bair Hugger
▫️ Limited monitoring: minimum safe setup
- Wrap up Materials
1️⃣4️⃣ 15 Advanced MCQs with Teaching Explanations
▫️ Includes airway emergencies, comorbidities, pain, physiology
1️⃣5️⃣ Summary Tables & Quick Reference
▫️ “Pediatric Anesthesia at a Glance” Poster
▫️ Normal vitals by age, drug doses, ETT size
▫️ Printable for OR walls or mobile screenshots
1️⃣6️⃣ Final Words
▫️ Reflection on caring for children
▫️ The mix of precision and compassion
▫️ Empowering anesthesiologists in every setting
📌 This guide is your reference when facing pediatric anesthesia — in every setting.
Stay structured. Stay vigilant. Act wisely. 🧠
1️⃣ Introduction to Pediatric Anesthesia
🎯 “Children are not small adults.” This is more than a saying — it's a safety principle.
🌟 Why Pediatric Anesthesia Deserves a Mastery Guide
- Pediatric physiology differs across age groups: neonates, infants, toddlers, children, and adolescents all react differently to anesthetics.
- Airway anatomy, drug metabolism, and cardiovascular reflexes require precise understanding and careful planning.
- High stakes, high sensitivity: Minor miscalculations in drug dosing or equipment can lead to serious complications.
- Family dynamics and emotional preparation add another layer of complexity to your anesthetic plan.
🔍 What Makes Pediatric Anesthesia Unique?
| Domain | Pediatric Difference |
|---|---|
| Airway | Larger tongue, floppy epiglottis, higher glottis, funnel-shaped larynx |
| Cardiovascular | Stroke volume fixed → HR-dependent CO |
| Respiratory | High O₂ consumption, lower reserve → faster desaturation |
| Pharmacokinetics | Immature liver/kidney → altered metabolism and clearance |
| Thermoregulation | Immature → higher risk of hypothermia |
🧠 Core Principles
- Think in age- and weight-based metrics for everything: drug dosing, equipment sizing, fluid therapy.
- Anticipate airway challenges even in routine cases.
- Always pre-check all drug calculations and ventilator settings — even if auto-calculated.
📌 Clinical Tip:
Always keep the resuscitation dose of adrenaline (10 mcg/kg) in mind. Emergencies in pediatrics escalate fast — be ready.
2️⃣ Preoperative Assessment in Pediatric Anesthesia
“More than weight and fasting — assess the whole child.”
📌 Why Pre-op Assessment Is Different in Pediatrics
In adult anesthesia, you assess history, comorbidities, airway, and labs.
In pediatric anesthesia, you assess:
- The child
- The parents
- The physiology by age
- And the behavior on the day of surgery
Children aren’t small adults. Their anatomy, psychology, pharmacology, and responses are age-specific — and so should be your assessment.
🔶 Key Components of Pediatric Preoperative Evaluation
| 🔍 Component | ✅ What to Assess |
|---|---|
| Age & Weight | Accurate weight in kg is essential for every calculation (drug, fluid, ETT). Use age to anticipate anatomy and behavior. |
| Developmental Stage | Neonate, infant, toddler, child, adolescent — each has unique needs and fears. |
| Feeding History | Preterm? Failure to thrive? Formula or breastfed? Risk of aspiration? |
| Medical History | Congenital anomalies, cardiac defects, asthma, epilepsy, metabolic disease |
| Surgical History | Previous anesthesia? Intubation issues? Apnea in neonates after surgery? |
| Medications & Allergies | AEDs, inhalers, steroids, herbal remedies |
| Recent Illness | URTI, LRTI, fever, COVID — always note desaturation risk, reactive airways |
| Vaccination & Infection Risk | Unvaccinated? RSV season? Check for post-viral inflammation risk |
🧠 Age-Based Risk Awareness
| 🧒 Age Group | Key Concerns |
|---|---|
| Neonates (<28d) | Immature liver/kidney, apnea risk, hypoglycemia, cold stress |
| Infants (1-12m) | Separation anxiety, difficult IV access, hypoxia risk |
| Toddlers (1–3y) | Fear, crying, URTI common, bradycardia risk on induction |
| Preschoolers (3–6y) | Curious, may cooperate; prone to laryngospasm |
| School-age & Adolescents | Modest, may hide history; higher tolerance to stressors |
📋 Essential Pre-op Questions (Quick Checklist)
- ❓ Has your child had anesthesia before? Any problems?
- ❓ Has your child been sick recently? (cold, fever, wheezing?)
- ❓ Does your child have any known heart or lung conditions?
- ❓ How much does your child weigh (exactly)?
- ❓ Has your child ever stopped breathing after surgery (apnea)?
- ❓ Is your child on any regular medications?
- ❓ Do you or any family members have issues with anesthesia (e.g. MH)?
⏳ Fasting Guidelines (Clear Table)
| Age | Solids | Breast Milk | Clear Fluids |
|---|---|---|---|
| <6 months | 6 hours | 4 hours | 2 hours |
| >6 months | 6 hours | 4 hours | 2 hours |
🔺 In resource-limited areas, clarify when the last meal was and document it clearly.
Never assume fasting was done correctly — always verify!
📌 Clinical Tips
- 🩺 Always auscultate the chest before induction — especially in toddlers.
- 🧴 Check skin folds and IV access sites in advance — fragile or difficult?
- 🧼 Ensure parents understand fasting clearly and confirm consent in layman's language.
- 💬 Reassure the child and parent — with age-appropriate words and calm body language.
🧸 Parent–Anesthetist Interaction Is Part of the Exam
Your confidence and clarity directly affect how calm the parent is — which affects the child’s behavior. Consider this your first anesthetic.
3️⃣ Pediatric Airway & Equipment Sizing
“Your tube size is not a guess — it’s a lifesaver.”
🧠 Pediatric Airway: How It Differs from Adults
Understanding pediatric airway anatomy is the foundation of safe anesthesia. Failure to anticipate these differences leads to hypoxia, trauma, or failed intubation.
| Feature | Pediatric vs. Adult |
|---|---|
| Tongue | Larger relative to mouth — risk of obstruction |
| Epiglottis | Long, floppy, omega-shaped |
| Larynx | Anterior and cephalad (C3–C4) vs. adult (C5–C6) |
| Narrowest Part | Cricoid cartilage (vs. glottis in adults) |
| Neck Flexibility | Higher risk of airway collapse and loss of alignment |
🔺 In infants and neonates, even minor airway swelling = major obstruction.
📐 Estimating ETT Size — Amir’s Formula Highlighted 💎
✅ Uncuffed ETT Size = (Age in years ÷ 4) + 4
✅ Cuffed ETT Size = (Age ÷ 4) + 3.5 (Used in most modern settings)
✅ ETT Depth = (Age ÷ 2) + 12 (oral) OR 3 × ETT size
📊 Master Table: Airway Equipment by Age & Weight
| Age | Weight (kg) | ETT Size (mm) | Depth (cm) | LMA Size | Blade |
|---|---|---|---|---|---|
| Preterm (<2.5 kg) | ~2.0 | 2.5–3.0 uncuffed | 7–8 | — | Miller 0 |
| Newborn | 3.0 | 3.0–3.5 uncuffed | 8–9 | 1 | Miller 0–1 |
| 6 months | 7.0 | 3.5–4.0 | 9–10 | 1.5 | Miller 1 |
| 1 year | 10 | 4.0 | 10–11 | 1.5 | Miller 1 |
| 2–3 years | 12–15 | 4.5 | 11–12 | 2 | Miller 1–2 |
| 4–6 years | 16–20 | 5.0 | 13–14 | 2.5 | Miller 2 / Macintosh 1 |
| 7–10 years | 21–30 | 5.5–6.0 | 15–17 | 3 | Macintosh 2 |
| >10 years | >30 | 6.0–7.0 | 18+ | 3–4 | Macintosh 2–3 |
📌 Color-code for OR wall poster:
- 🔵 Neonate
- 🟢 Infant
- 🟡 Toddler
- 🟠 Child
- 🔴 Adolescent
🎯 Clinical Reminders:
- ✅ Always check the mark at the lip after intubation — document it.
- ✅ Cuffed tubes are preferred in modern practice with minimal leak and proper monitoring.
- ✅ Leak test before extubation — especially in prolonged cases.
- 🔺 Down syndrome, Pierre Robin, or cleft palate = Prepare for difficult airway.
📉 Case Highlight: Sudden Desaturation in a 2-year-old
Scenario: Post-intubation, child desats to 80%.
✅ Tube confirmed at 12 cm
✅ No breath sounds on the left
🎯 Diagnosis: ETT too deep → Right mainstem bronchus
🛠️ Fix: Withdraw 1–2 cm and reassess — lungs re-expand.
🧰 Equipment Preparation Checklist
Before you induce:
- [ ] Age- and weight-appropriate ETTs (2 sizes up/down)
- [ ] LMA (backup airway)
- [ ] Suction, syringe for cuff inflation
- [ ] Lubricant, stylet if needed
- [ ] Bag-mask & oxygen ready
- [ ] Plan B: GlideScope, bougie, or supraglottic backup
🧵 Always check & prepare airway gear before any IV attempt in a child.
4️⃣ Drug Dosing in Pediatrics — Safe, Sharp, and Structured
“Every mg must be deliberate. Every ml must be double-checked.”
🌟 Pediatric Pharmacology at a Glance
Children’s bodies distribute, metabolize, and excrete drugs differently than adults. These differences change with:
- Age (organ maturity)
- Body water and fat content
- Plasma protein levels
- Liver enzyme development
❗ Neonates and infants are NOT just tiny adults — overdosage and underdosage are both dangerous.
📊 Master Table: Common IV Drugs in Pediatric Anesthesia
| Drug | Dose (mg/kg) | Notes |
|---|---|---|
| Ketamine | 1–2 IV / 4–6 IM | Hemodynamically stable; good for induction without IV |
| Propofol | 2–3 | Neonates more sensitive → start lower; avoid in unstable infants |
| Thiopental | 3–5 | Rarely used now, but know it for exams |
| Midazolam | 0.05–0.1 | Sedation; slow push, esp. in neonates |
| Fentanyl | 1–2 mcg/kg | Synergistic with sevoflurane; apnea risk at high dose |
| Morphine | 0.05–0.1 | Avoid in neonates (immature clearance) |
| Remifentanil | 0.1–0.5 mcg/kg/min | Excellent for short, intense procedures |
| Tramadol | 1–2 | Avoid in <1 yr due to CYP metabolism variability |
| Paracetamol | 10–15 | IV or PR; beware cumulative dose |
| Atracurium | 0.5 | Hofmann elimination → safe in renal/liver issues |
| Rocuronium | 0.6–1.2 | Ideal for RSI; reversed with sugammadex if available |
| Suxamethonium | 1–2 | Only for rapid control (e.g. laryngospasm) |
| Neostigmine | 0.05 + Atropine/Glyco | For reversal — glycopyrrolate preferred |
| Dexamethasone | 0.1–0.5 | For airway edema or antiemesis |
| Ondansetron | 0.1 | Routine for tonsil/adenoid cases |
💡 Formulas You Must Remember
| Clinical Use | Formula |
|---|---|
| ETT Size | (Age ÷ 4) + 4 (uncuffed) |
| ETT Depth (oral) | (Age ÷ 2) + 12 |
| Fluid rate | 4-2-1 rule (see below) |
| Glucose needs | Neonates: 4–6 mg/kg/min |
🚰 Maintenance Fluids: The “4–2–1 Rule”
| Weight | Fluid Rate |
|---|---|
| First 10 kg | 4 ml/kg/hr |
| Next 10 kg | 2 ml/kg/hr |
| >20 kg | 1 ml/kg/hr |
🧃 Preferred fluid: Dextrose 0.45% NS with K+ (if NPO >6–8 hrs)
Avoid NS alone in neonates → risk of hyperchloremic acidosis
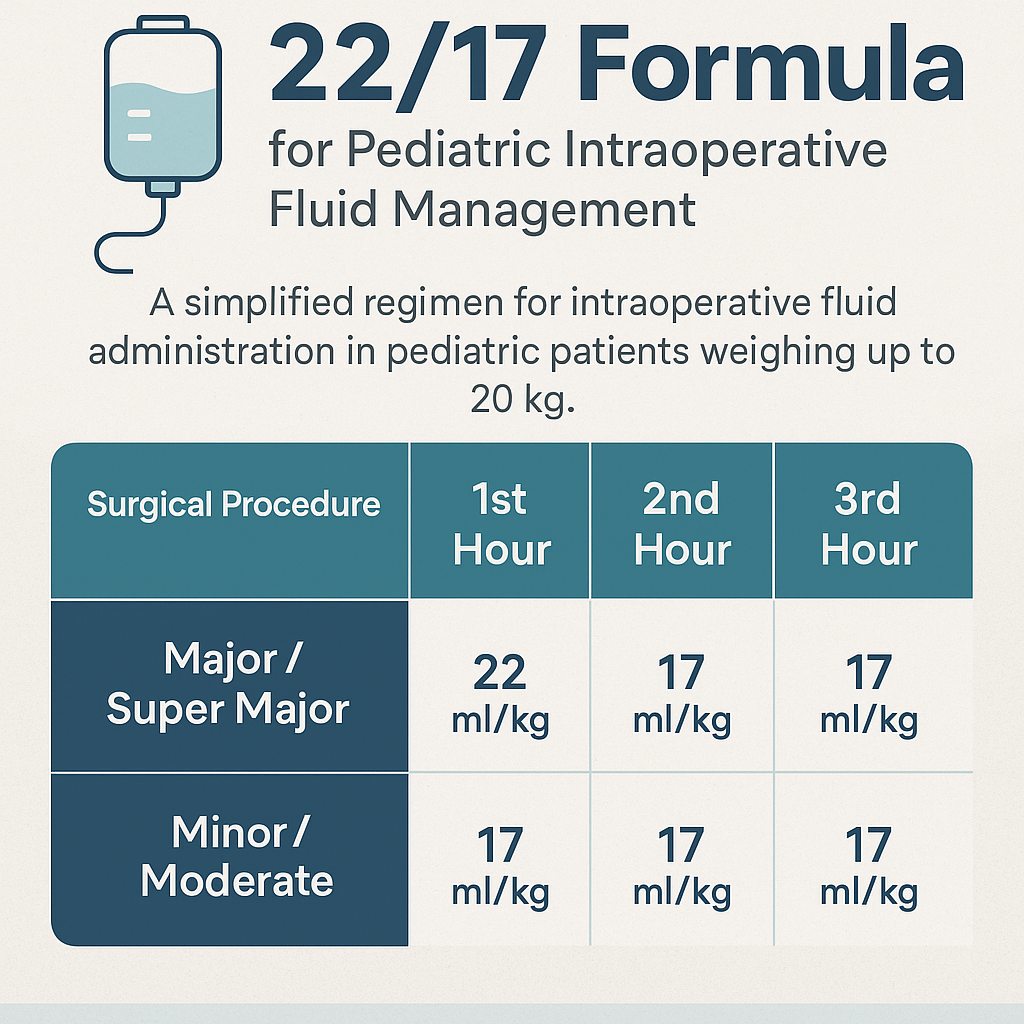
🧭 22/17 Formula — Simplified Pediatric Fluid Strategy
A practical, hour-based formula for intraoperative IV fluid management in children ≤20 kg or ≤5 years. It integrates fasting deficit, maintenance, and third-space losses into one clear hourly plan.
Ideal for both high- and low-resource settings.
🖋️ Developed by Dr. Riyadh Khudeir Hamed, Pediatric Anesthesiologist – Baghdad Medical Complex, Iraq.
🧸 Special Considerations
| Patient Type | Tip |
|---|---|
| Neonate | Reduce doses; slow metabolism & excretion |
| Infant with cold | Avoid high opioid dosing → laryngospasm, apnea |
| Cardiac patient | Avoid drugs that ↓ SVR or ↑ HR drastically |
| Syndromic child | Check for epilepsy → avoid ketamine/methohexital |
🔥 Red Flag: Underdose or Overdose?
🚨 Giving full adult induction dose to a 10-kg child = respiratory arrest
Always calculate by weight, double-check with a colleague, and draw up in clearly labeled syringes.
📌 Clinical Tip: Color-Coded Syringes & Tape
In many pediatric ORs, syringes are color-coded for safety.
If unavailable, label every syringe manually with drug + dose in mg/ml.
In resource-limited setups: Pre-calculate and write out dose ranges on the drug tray — especially for resuscitation drugs like adrenaline, atropine, and sux.
🧰 🔧 Limited-Resource Consideration: Maintenance Fluids in Pediatrics
In ideal settings, maintenance IV fluids are:
🧃 Dextrose 0.45% Normal Saline + 10–20 mmol/L KCl
But in many hospitals — especially district or rural — the options are limited.
✅ If Only 5% Dextrose in 0.9% NS (500 mL) Is Available:
Problem:
0.9% NS is hypertonic and high in sodium/chloride for maintenance — risk of:
- Hypernatremia
- Hyperchloremic metabolic acidosis
- Volume overload in neonates
Solution:
🔹 Dilute it if possible: Mix 250 mL D5NS + 250 mL Sterile Water → approximate D5 + 0.45% NaCl
🔹 If no dilution possible, limit rate, monitor sodium & chloride closely
🔹 Prefer enteral hydration as soon as tolerated
✅ If KCl Is Unavailable:
Potassium is vital — especially for NPO >6 hrs, vomiting, or surgical stress.
Options:
- Use Ringer’s Lactate (RL) or Plasmalyte if available → they contain ~4 mEq/L of K⁺
- Add banana/salty water by NG in extreme situations (not ideal, but documented in field medicine)
- Monitor ECG for hypokalemia signs (flattened T waves, U waves, arrhythmia risk)
✅ Can You Use Ringer’s Lactate with Dextrose?
Yes — but mix must be prepared manually (e.g. 250 mL RL + 250 mL D5W)
⚠️ Watch for precipitation risk if mixing with certain drugs (e.g. calcium + phosphate combos)
🔴 Clinical Red Flag:
Avoid giving Dextrose 5% in Ringer’s as a bolus — risk of hyponatremia and rebound hypoglycemia
Only use as maintenance in stable patients.
📌 In Summary: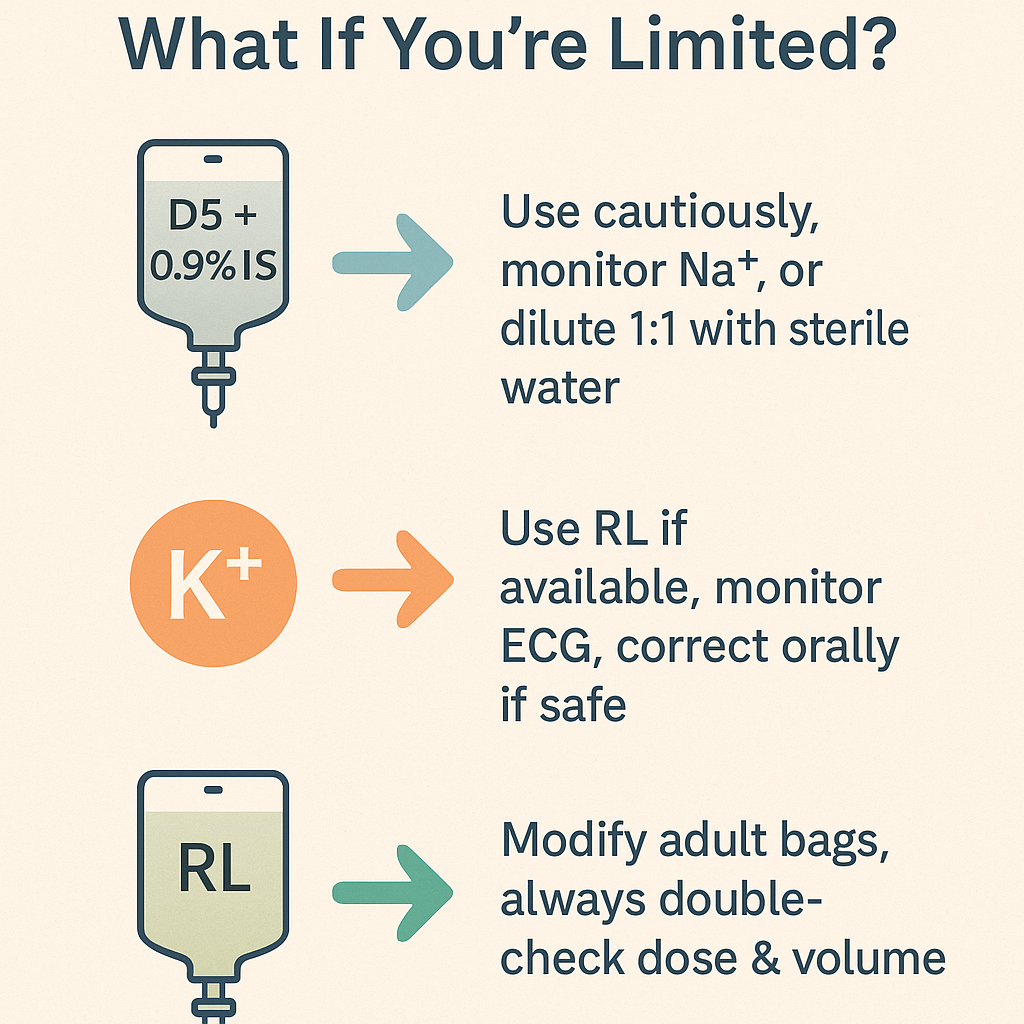
✨ Pediatric anesthesia is not about perfection — it’s about precision within your means.
5️⃣ Induction Techniques in Pediatric Anesthesia
“Fast, calm, and safe — your first touch sets the tone.”
🎯 Choosing Between Inhalational and IV Induction
| Approach | Preferred In... | Notes |
|---|---|---|
| Inhalational | Most children aged 6 months–6 years | Fear of needles, easy to mask, rapid onset |
| IV Induction | Older children or already cannulated | Precise control, faster airway reflex suppression |
| IM Ketamine | Emergencies, uncooperative child, no IV | Useful in field work, seizures, combative behavior |
🌀 Inhalational Induction — Step by Step (Sevoflurane)
- Prepare circuit: Fill vaporizer with sevoflurane. Prime the circuit with 8% sevo and 100% O₂.
- Apply mask: Gently place on a calm, semi-awake child.
- Maintain calm: Don’t rush — children sense panic.
- Observe for signs: Apnea, limpness, eye deviation = time to reduce to 2–3% and secure IV access.
- Insert IV: After loss of reflexes. Proceed to airway management.
🛡️ Avoid halothane unless no other option — risk of bradycardia and arrhythmia.
💉 IV Induction — Doses and Pearls
- Fentanyl: 1–2 mcg/kg → Blunts sympathetic response
- Midazolam: 0.05–0.1 mg/kg → Good for anxious older child
- Propofol: 2–3 mg/kg (reduce in neonates)
- Ketamine: 1–2 mg/kg (especially if no IV = IM 4–6 mg/kg)
✅ Start with fentanyl or midazolam before propofol for smoother induction
❗ Be cautious with ketamine if child has full stomach or elevated ICP
🚨 Trouble Points During Induction
| Situation | What to Do |
|---|---|
| Laryngospasm | Stop stimulation, deepen anesthesia, jaw thrust + CPAP; if persists → IV sux 0.5–1 mg/kg |
| Bradycardia | Esp. with halothane or hypoxia → Give atropine 20 mcg/kg IV/IM |
| Crying/Struggling | Avoid forcing — go slowly, reassure; if needed, switch to ketamine IM |
| Breath-holding | Common with fear — allow time, coach child, avoid rushing |
✨ Induction Tips by Age
| Age Group | Best Method | Key Advice |
|---|---|---|
| Neonate | IV with fentanyl + low-dose propofol/ketamine | Risk of apnea and hypothermia |
| Infant (1–12m) | Inhalational preferred | Monitor glucose, temp, O₂ |
| Toddler | Sevo mask induction | Crying → use distraction toys, cartoons, music |
| School-age | IV or Sevo | Involve them in the process, give choices |
| Adolescent | IV induction | Respect modesty, clear explanation, anxiolysis helpful |
🌍 Limited-Resource Settings
- If no sevoflurane → Use halothane 1–2% with caution
- No pediatric IV cannulas? → Use 24G butterfly or scalp vein set
- No prefilled syringes? → Draw and label all syringes in advance
- If no IM ketamine? → Nebulized midazolam or oral ketamine (off-label, low-dose)
📌 Real-World Example
A 2-year-old with URTI and wheeze arrives for emergency hernia surgery.
✅ Choose IV ketamine 1–2 mg/kg for bronchodilation and stable hemodynamics
✅ Avoid sevoflurane if wheezing
✅ Have suction, atropine, and ambu-bag ready
🧠 “The best induction is the one that keeps the child safe — not just the smoothest.”
6️⃣ Maintenance & Monitoring in Pediatric Anesthesia
“Once asleep, the real work begins.”
🔧 Goals of Maintenance
- Maintain adequate depth of anesthesia
- Ensure hemodynamic and respiratory stability
- Preserve normothermia, normoglycemia, and oxygenation
- Be ready to treat any complication — early and fast
💨 Maintenance Agents — What to Use and When
| Agent | Dose / % | Notes |
|---|---|---|
| Sevoflurane | 1.5–3% | Gold standard in pediatrics; fast on/off, minimal airway irritation |
| Halothane | 0.5–1% | Use only if no sevo; bradycardia and arrhythmia risk |
| TIVA (Propofol infusion) | 100–150 mcg/kg/min | Older children or day-case; not preferred in neonates |
| N₂O (Nitrous Oxide) | Up to 70% | Reduces MAC of sevo; avoid in bowel cases, shunts, pneumothorax |
🛡️ Safety Pearls
- 🎈 Use air + O₂ mix unless hypoxia risk is high — pure O₂ = absorption atelectasis risk
- 🧪 Avoid prolonged high-dose sevo in infants → theoretical risk of neurotoxicity
- 🧊 Actively warm the child if <32 kg — they cool fast
- 🍬 If fasting >8 hrs, give dextrose infusion or check glucose hourly
📟 Monitoring Parameters
| Parameter | Goal Range | Notes |
|---|---|---|
| HR | Age-appropriate | Tachycardia = pain/light; Bradycardia = hypoxia/drug |
| BP | Within 20% of baseline | Hypotension = sevo/propofol overdose, blood loss |
| SpO₂ | >94% | Desaturation = secretions, laryngospasm, disconnection |
| EtCO₂ | 35–45 mmHg | Low = overventilation; High = hypoventilation or CO₂ retention |
| Temp | 36.0–37.5°C | Hypothermia is common! Use Bair Hugger or warm IV fluids |
| BG (if <1 yr) | 70–150 mg/dL | Hypoglycemia can be silent — check every 1–2 hrs if NPO |
🔍 Ventilation Strategy — General Guide
| Age | Mode | Tidal Volume (ml/kg) | RR |
|---|---|---|---|
| Neonate | Pressure control | 6–8 | 30–40 |
| Infant | PC or VCV | 6–8 | 25–35 |
| Toddler | VCV | 6–8 | 20–30 |
| >5 years | VCV | 6–8 | 16–25 |
🎯 Always watch EtCO₂ trend, not just the number
🎯 Avoid auto-PEEP — small lungs = fast trap
🔌 Devices That Help (If Available)
| Monitor | Benefit |
|---|---|
| EtCO₂ | Airway patency, ventilation status |
| BIS Monitor | Depth of anesthesia, especially with TIVA |
| NIRS (near-infrared spectroscopy) | Brain oxygenation — especially in neonates/cardiac cases |
| Precordial stethoscope | Old but gold — early hypoventilation or laryngospasm detection |
🌍 Low-Resource Adaptations
- ❌ No EtCO₂? → Watch RR + chest rise + O₂ sat + precordial sounds
- ❌ No temperature probe? → Touch hands/feet, check for cool limbs
- ❌ No infusion pump? → Use burette or hourly recalculated drip
- ✅ No TIVA setup? → Stick with Sevo + Fentanyl maintenance
- ✅ No NIRS? → Keep MAP in range and avoid hypocapnia
💡 Remember:
🧠 Children desaturate, cool, and drop BP faster than adults.
The key is to stay ahead — not just react.
7️⃣ Emergence & Postoperative Care in Pediatrics
“Safe sleep is just the start — smooth waking is your true test.”
🎯 Goals of Emergence
- Maintain airway patency
- Ensure adequate spontaneous ventilation
- Prevent airway complications (e.g. laryngospasm)
- Alleviate pain, agitation, nausea
- Ensure a calm transition to recovery
😴 Deep vs. Awake Extubation — What to Choose?
| Approach | Best For | Risk | Tip |
|---|---|---|---|
| Deep Extubation | URTI, reactive airways | Obstruction, aspiration | Only if no residual muscle blockade |
| Awake Extubation | Vomiting risk, full stomach | Bucking, coughing | Suction well, ensure consciousness & tone |
✅ Always ensure full reversal of NMB (Train-of-four >0.9 if monitored)
✅ Suction the oropharynx before removing tube
🛑 Common Post-op Complications & Management
| Complication | Sign | Management |
|---|---|---|
| Laryngospasm | High-pitched stridor, chest wall retraction, desaturation | 100% O₂ + jaw thrust + CPAP → IV sux 0.5–1 mg/kg |
| Emergence Delirium | Disorientation, thrashing, inconsolable crying | Rule out pain → Give midazolam 0.05 mg/kg or fentanyl |
| Apnea (neonates) | Pause in breathing >20 sec or bradycardia | Stimulate, support airway, may need postop monitoring |
| Vomiting | Nausea, retching | Ondansetron 0.1 mg/kg IV |
| Pain | Tachycardia, crying, grimace | Use multimodal analgesia (see Section 12) |
🧠 Pediatric Recovery Priorities
| System | Focus |
|---|---|
| Airway | Stridor, retractions, suctioning needed? |
| Breathing | RR, SpO₂, EtCO₂ if monitored |
| Circulation | HR, BP, perfusion, temperature |
| Neurologic | Responsiveness, movement, crying |
| Pain/Nausea | FLACC scale, parental input helpful |
💡 Clinical Tips
- 👶 Preterms & ex-preterms <60 weeks: Risk of apnea → observe ≥12 hrs postop
- 🧬 Syndromic kids: May have airway collapse or secretions → stay close
- 💉 Re-dose dexamethasone + ondansetron in high-risk vomiting cases (e.g. T&A)
🌍 Limited-Resource Recovery Setup
- ✅ Pulse oximetry is non-negotiable
- ❌ No monitor? → Observe breathing pattern, color, and movement continuously
- 🧴 Keep suction, O₂ source, and self-inflating bag ready at bedside
- ❗ Keep Atropine, Sux, and Naloxone/Naluphine drawn up and labeled
🧸 Parent Communication in PACU
Let them see their child once stable.
Use calming phrases:
“They’re waking up well. Crying is a good sign of recovery.”
“We’re keeping them safe and comfortable until you can go home.”
8️⃣ Emergency Troubleshooting in Pediatric Anesthesia
“Things go wrong fast — your hands must move faster than your fear.”
🚨 What to Do When Things Go Wrong
Real-life, real-speed action steps for pediatric OR emergencies
💥 1. Laryngospasm
Trigger: Secretion, light anesthesia, URTI, extubation phase
Signs: Inspiratory stridor → silent chest → desaturation → bradycardia
🛠️ Management Checklist:
- Call for help 🚨
- 100% O₂ via tight-fitting mask
- Apply jaw thrust + CPAP (10–15 cm H₂O)
- Deepen anesthesia (IV Propofol or Sevo mask)
- If persists:
- IV Suxamethonium 0.5–1 mg/kg
- If no IV: IM Sux 4 mg/kg
- Intubate if required
🔺 Always suction before extubation in at-risk children.
💓 2. Bradycardia in Neonates & Infants
Trigger: Hypoxia, halothane, vagal response (intubation, suction)
🛠️ Management:
- First: Fix oxygenation!
- Then: IV Atropine 20 mcg/kg (repeat once if needed)
- If no IV: IM Atropine
- Consider chest compressions if HR <60 + poor perfusion
✅ If on halothane → switch to 100% O₂ + remove volatile
😷 3. Inhalational Induction Gone Bad
Trigger: Crying, struggling child → breath-holding, desaturation
🛠️ Rescue Plan:
- Stop sevo, ventilate with 100% O₂
- If bradycardia → give Atropine
- If breath-holding continues → IV/IM ketamine 1–2 mg/kg
- Consider aborting and reattempting with IV or IM induction
💉 4. IV Access Failure in Small Children
Scenario: Can’t get a line, child is crying, inhalation not deep enough
🛠️ Plan B Options:
- IM Ketamine 4–6 mg/kg — safe, rapid sedation
- Intraosseous (IO) Access — proximal tibia
- Scalp or dorsal foot veins in infants
- Use transillumination device if available
🔧 Pro tip: Always have EMLA cream or vapocoolant spray handy pre-op
🫁 5. Post-Intubation Desaturation
Causes:
- Mainstem intubation
- Obstruction (secretions, kinked ETT)
- Pneumothorax
- Disconnection
🛠️ Stepwise Approach:
- Confirm chest rise, auscultate both lungs
- Withdraw ETT slightly if breath sounds absent on left
- Suction if secretions audible
- Check EtCO₂ and bag compliance
- Rule out tension pneumothorax (hyperresonance, tracheal shift)
✨ Always document ETT depth and size clearly in the chart
📌 Emergency Drugs Cheat Sheet (mg/kg)
| Drug | Dose | Notes |
|---|---|---|
| Suxamethonium | 1 (IV), 4 (IM) | Laryngospasm |
| Atropine | 20 mcg/kg | Bradycardia, vagal events |
| Adrenaline | 10 mcg/kg | Cardiac arrest, anaphylaxis |
| Ketamine (IM) | 4–6 | When no IV access |
| Midazolam | 0.05–0.1 | Seizures or agitation |
🧠 Tips to Stay Ahead
-
Keep an Emergency Tray pre-filled with:
✅ Sux
✅ Atropine
✅ Adrenaline
✅ Naloxone
✅ Glucose 10% -
Label every syringe clearly
-
Never hesitate to call for help early — children can deteriorate silently
9️⃣ Mini Surgical Playbooks — Pediatric OR at a Glance
“Each surgery has its rhythm — learn it, play it, master it.”
🔹 1. Inguinal Hernia Repair (especially in ex-preterm infants)
| Step | Note |
|---|---|
| Pre-op | Assess for post-op apnea risk if <60 weeks post-conception age → may need overnight monitoring |
| Induction | Sevo or ketamine; IV preferred if available |
| Airway | LMA or ETT depending on case and reflux risk |
| Analgesia | Caudal block or local infiltration; add acetaminophen |
| Post-op | Monitor for apnea, bradycardia, especially in ex-premature infants |
🔹 2. Circumcision
| Step | Note |
|---|---|
| Pre-op | Ensure parental consent for block-only if no GA |
| Induction | Often no GA needed — penile block (dorsal nerve + ring block) is enough |
| Airway | If GA: mask or LMA usually sufficient |
| Analgesia | Penile block + paracetamol |
| Post-op | Reassure parents re: mild bleeding and discomfort |
🧠 Ideal for low-resource ORs with trained regional skills and no vaporizers.
🔹 3. Tonsillectomy / Adenoidectomy
| Step | Note |
|---|---|
| Pre-op | High bleeding risk; check Hb, screen for OSA |
| Induction | IV or inhalational; secure ETT with cuff |
| Airway | Cuffed ETT with throat pack; note depth carefully |
| Analgesia | Avoid high opioids → risk of airway obstruction in PACU; dexamethasone + paracetamol ± low-dose fentanyl |
| Post-op | Watch for bleeding, vomiting, airway edema → observe minimum 4–6 hrs |
✨ Pro Tip: Avoid morphine in OSA or obese children — use non-opioid adjuncts.
🔹 4. Appendectomy (Open or Laparoscopic)
| Step | Note |
|---|---|
| Pre-op | Is child stable? Fluid resuscitation done? NPO? |
| Induction | RSI if perforated or vomiting — ketamine or fentanyl + propofol + rocuronium |
| Airway | Cuffed ETT; secure well for Trendelenburg/laparoscopy |
| Analgesia | Paracetamol + caudal/TAP block + IV opioid |
| Post-op | Watch for pain, ileus, fever; continue IV fluids for 12–24 hrs |
🔹 5. VP Shunt Insertion (Hydrocephalus)
| Step | Note |
|---|---|
| Pre-op | Risk of raised ICP — vomiting, headache, lethargy |
| Induction | Avoid ketamine; use propofol or thiopental |
| Airway | Cuffed ETT; careful head positioning |
| Analgesia | IV paracetamol + fentanyl; avoid deep sedation post-op |
| Post-op | Position head 15–30° up; monitor consciousness and pupils closely |
🚨 Sudden agitation or vomiting post-op may = shunt malfunction or bleed
💡 Clinical Teaching Tip
Use these playbooks during pre-induction timeout:
“Today’s surgery is T&A in a 5-year-old with mild OSA. I’ll avoid morphine, use dexamethasone, and extubate fully awake.”
🔟 Perioperative Challenges in Pediatric Comorbidities
“Their syndromes may be rare — but their safety is never negotiable.”
Comorbidities and syndromic features in children demand vigilant assessment, careful drug selection, and a tailored anesthesia plan. Whether it's a cardiac shunt, fragile airway, or post-viral wheeze, your foresight prevents catastrophe.
❤️ A. Congenital Heart Disease (CHD)
“The heart is imperfect, but your plan must be flawless.”
🩺 Common Lesions by Type
| Left-to-Right Shunts | VSD, ASD, PDA, AV canal |
|---|---|
| Right-to-Left Shunts | TOF, Eisenmenger, Single ventricle |
| Obstructive Lesions | Coarctation of aorta, pulmonary stenosis |
| Cyanotic Complexes | Transposition of great vessels, truncus arteriosus |
📌 Pre-op Musts
- Echo report: VSD size, pulmonary pressures, ventricular function
- Functional status: feeding tolerance, weight gain, activity level
- Oxygen saturation trend: baseline? Cyanotic spells?
- Hematocrit / Hb: risk of hyperviscosity in chronic hypoxia
- Consider RSV prophylaxis, endocarditis risk, fluid status
- Check current meds: Diuretics, ACEi, Digoxin?
🛠️ Anesthetic Goals
| Goal | Rationale |
|---|---|
| Maintain SVR | Prevent reversal of shunt in R→L lesions (e.g. TOF) |
| Avoid hypoxia & acidosis | These ↑ PVR → worsens R→L shunt |
| Preserve preload & contractility | Avoid drugs that depress myocardium |
| Control PVR | Avoid high airway pressures, hypothermia, hypercarbia |
💉 Induction Strategy
| Agent | Rationale |
|---|---|
| Ketamine | Ideal for TOF, Eisenmenger: ↑ SVR & CO |
| Fentanyl | Smooths response to intubation, ↓ stress |
| Avoid high-dose propofol or thiopental | Risk of ↓ SVR → shunt worsening, arrest |
| Rocuronium or Atracurium | Safe, stable hemodynamics |
If no IV access → IM Ketamine is acceptable in cyanotic lesions
🌬️ Monitoring During Surgery
| Monitor | Use |
|---|---|
| Preductal SpO₂ (right hand) | Cerebral oxygenation |
| Postductal SpO₂ (foot) | Detect differential cyanosis |
| Invasive BP | Useful in unstable or single-ventricle physiology |
| EtCO₂ + ABG | Detect ventilation mismatch, rising PVR |
🧊 Intra-op Pearls
- Warm the child actively (hypothermia ↑ PVR)
- Avoid overhydration (risk of CHF in large VSD/PDA)
- Use 100% O₂ if saturation drops, but titrate FiO₂ in single-ventricle physiology
- Phenylephrine preferred over ephedrine for hypotension → supports SVR
🩹 Post-op Priorities
| Focus | Details |
|---|---|
| Oxygenation | Titrate based on baseline SpO₂; don’t chase 100% in cyanotics |
| Fluids | Cautious maintenance; avoid overload |
| Temperature | Maintain normothermia |
| ICU Monitoring | Some may need ventilatory or inotrope support post-op |
| Early signs of decompensation | Poor perfusion, lethargy, cyanosis, tachypnea |
🔑 Final Tips
-
TOF = Tet spells may be provoked by crying or surgical stress → treat with:
- 100% O₂
- Knees-to-chest position
- Morphine 0.1 mg/kg
- Phenylephrine
- Volume bolus
- Beta-blocker if refractory (e.g., propranolol)
-
Eisenmenger physiology is fragile → high mortality under GA → if elective, defer to tertiary center
🫁 B. Respiratory Illness (URTI, LRTI, Asthma, RSV)
“Even a cold can kill — never underestimate a child with URTI or LRTI.”
🔴 Postpone surgery if:
- Fever >38°C
- Wet or productive cough
- SpO₂ <95% at rest
- Audible wheeze, rales, or increased work of breathing
- Recent hospitalization for RSV (last 4–6 weeks)
⚠️ Persistent symptoms beyond 2 weeks? → Suspect post-viral hyperreactivity
➡️ Proceed only with caution, bronchodilator prep, and deep anesthesia.
🔶 If Surgery Must Proceed (Urgent Cases):
✅ Glycopyrrolate to dry secretions
✅ Pre-op bronchodilators (salbutamol)
✅ Deep plane of anesthesia
✅ Avoid LMA — use cuffed ETT
✅ Extubate deep or fully awake — never in-between
✅ PACU monitoring for at least 4–6 hours
🧠 URTI → laryngospasm risk
🧠 LRTI → desaturation and airway reactivity risk
🛡️ Protective Strategy for Anesthesia
🔹 Preoperative Phase
- Glycopyrrolate 5–10 mcg/kg IV/IM
- Salbutamol via MDI/spacer or nebulizer (before induction)
- Nebulized epinephrine 0.5 ml/kg of 1:1000 in 3 ml NS if stridor
- Rebrief your team about extubation plan and airway rescue readiness
🔹 Induction
| Component | Strategy |
|---|---|
| Route | Prefer IV induction to avoid coughing, struggling |
| Agents | Propofol + fentanyl OR ketamine if IV access is available; Sevoflurane only if needed |
| Depth | Ensure deep anesthesia before airway manipulation |
| Avoid | LMA → increases risk of laryngospasm in inflamed airways |
🔹 Airway Management
- Use cuffed ETT with appropriate leak at 20–25 cmH₂O
- Minimize laryngoscopy attempts
- Lubricate ETT well
- Use video laryngoscope if available
- Suction (oral + nasal) ready at all times
🔹 Maintenance Phase
- Use humidified gases when possible
- Monitor EtCO₂ for ventilation status
- Avoid dry soda lime → reduces airway irritation
- Minimize manipulations and positioning that stimulate the airway
🔹 Extubation Strategy
| Type | When to Use |
|---|---|
| Deep | No secretions, no reflux risk, smooth course |
| Awake | Secretions present, multiple airway attempts, full stomach |
💉 Premedicate before extubation:
- Glycopyrrolate
- IV Lidocaine 1 mg/kg
🔹 Post-op Monitoring
- Position child semi-upright
- Administer oxygen via nasal cannula or face mask
- Observe for:
- Stridor
- Retractions
- Desaturation
- Apnea
🧪 If post-extubation stridor:
➡️ Nebulize salbutamol or racemic epinephrine immediately
➡️ Extend PACU observation, especially for infants and ex-preterms
📌 Clinical Pearls
- URTI increases laryngospasm risk 10-fold
- LRTI can lead to bronchospasm, hypoxia, and apnea
- RSV can cause subglottic edema and wheeze for up to 6 weeks
- Ketamine is preferred over sevoflurane in secretory or reactive airways
🌍 Limited-Resource Adaptations
| Limitation | Practical Alternative |
|---|---|
| No nebulizer | Use salbutamol MDI into mask during inspiration |
| No glycopyrrolate | Atropine 10 mcg/kg (but CNS effects) |
| No humidifier | Add sterile NS drops into breathing limb |
| No EtCO₂ | Monitor chest rise, RR, SpO₂, auscultation closely |
🧠 C. Neurological & Syndromic Children
“Behind every syndrome is a fragile airway, a silent seizure, and a story you must respect.”
Children with neurological disorders or syndromes pose unique perioperative risks. Their comorbidities often span airway anomalies, aspiration risk, muscle tone abnormalities, and seizure susceptibility. Some syndromes bring multiple red flags — your pre-op vigilance is the most important anesthetic.
🧬 Common Conditions and Anesthetic Implications
| Condition | Anesthetic Challenges |
|---|---|
| Cerebral Palsy (CP) | Spasticity, GERD, aspiration risk, epilepsy, difficult IV access |
| Down Syndrome (Trisomy 21) | Macroglossia, atlanto-axial instability, congenital heart disease |
| Epilepsy / Seizure Disorders | Drug interactions, prolonged sedation, risk of breakthrough seizures |
| Hydrocephalus / VP Shunt | Elevated ICP, bradycardia risk, head positioning |
| Pierre Robin / Treacher Collins | Micrognathia, glossoptosis → severe airway difficulty |
| Muscular Dystrophies / SMA | Risk of MH-like reactions, prolonged paralysis, aspiration risk |
| Autism Spectrum Disorders | Unpredictable behavior, extreme sensitivity, limited cooperation |
🧠 Preoperative Checklist
- Developmental level and ability to cooperate
- History of seizures — frequency, medications, triggers
- Nutritional status, feeding difficulties
- Recent chest infections or aspiration episodes
- Cervical spine X-ray (in Down syndrome)
- Ventricular shunt function (for hydrocephalus)
- Drug list: AEDs, muscle relaxants, anti-reflux meds
🔺 Ask about previous anesthesia experience and airway difficulties.
💉 Induction Strategy
| Goal | Strategy |
|---|---|
| Calm, non-traumatic start | Pre-med with midazolam or ketamine (IN/IM if no IV) |
| Seizure safety | Continue AEDs; avoid enflurane, methohexital |
| Airway caution | Avoid forced mask ventilation in Pierre Robin, Down syndrome |
| GERD protection | RSI if aspiration risk (especially in CP, microcephaly) |
Preferred agents:
- Propofol or ketamine
- Fentanyl for hemodynamic blunting
- Rocuronium or atracurium (avoid sux in hypotonia or muscular dystrophies)
🌬️ Airway Management
| Syndrome | Airway Plan |
|---|---|
| Pierre Robin, Treacher Collins | Prepare for fiberoptic or LMA rescue, consider awake intubation if older |
| Down syndrome | Gentle neck handling, possible cervical collar, size down on ETT |
| CP, epilepsy | Routine airway with suction readiness (due to poor tone, secretions) |
🛠️ Always prepare:
- Video laryngoscope
- Supraglottic devices (LMA, iGel)
- Difficult airway cart and backup intubation tools
💊 Drug Safety in Neurologic Patients
| Drug | Comment |
|---|---|
| Midazolam | Excellent for anxiolysis but monitor for prolonged sedation in CP, epilepsy |
| Ketamine | Good for airway tone and seizure resistance |
| Propofol | Safe, short-acting — may be prolonged in AED use |
| Suxamethonium | Avoid in neuromuscular disorders (hyperkalemia risk) |
| Tramadol | Avoid in seizure-prone patients — lowers threshold |
| NSAIDs | Use with caution in CP with renal compromise or feeding issues |
🧊 Intraoperative Pearls
- Maintain normothermia
- Avoid excessive head rotation (especially in Down syndrome or shunted hydrocephalus)
- Monitor EtCO₂, HR, and ICP signs in hydrocephalus cases
- Document ETT depth and position carefully (anatomy may be distorted)
🩹 Post-op Recovery
| Risk | Management |
|---|---|
| Apnea or delayed emergence | Monitor closely in PACU; prolonged sedative effect in CP, epilepsy |
| Seizure | Treat promptly with midazolam or existing AED |
| Secretions / aspiration | Suction, upright positioning, early feeding restrictions |
| Pain / agitation | Use non-opioid agents + regional blocks if possible |
🧠 CP, autistic, and epileptic children may express pain as agitation — interpret wisely.
📌 Final Tips
- Children with syndromes often behave unexpectedly — your Plan B must be ready before induction.
- Many have unspoken histories — speak with parents, review old anesthesia records.
- Expect multiple anomalies in one child. Airway + cardiac + neuro + GI may all co-exist.
🕊️ “They may be fragile, but you must be firm in your vigilance — and gentle in your hands.”
🍽️ D. Gastrointestinal, Renal, & Metabolic Disorders
“Every ml, every mEq, every minute of fasting — it matters.”
These disorders may appear benign in the ward, but under anesthesia, they carry profound risks: aspiration, electrolyte derangement, drug accumulation, glucose instability, and acidosis. Your job is to uncover hidden vulnerabilities — and tailor every drop accordingly.
🧪 Common Conditions & Risk Highlights
| Condition | Main Risk |
|---|---|
| GERD / Hiatal Hernia | Aspiration during induction or emergence |
| Renal dysplasia / CKD | Electrolyte imbalance, altered drug clearance |
| Steroid-dependent illness (e.g., CAH) | Adrenal crisis if no peri-op steroids |
| Diabetes Mellitus / DKA | Hypo/hyperglycemia, acid-base disturbance |
| Inborn Errors of Metabolism | Hypoglycemia, lactic acidosis, ammonia crisis |
🔍 Preoperative Checklist
- NPO time — was the child fasting too long?
- Last meal composition — sugary? fatty? milk?
- Fluid and electrolyte status — vomiting? diarrhea?
- Current meds — insulin, bicarbonate, steroids, phosphate binders?
- Glucose level — check baseline and trends
- Metabolic profile or ABG if suspected acidosis
🧠 Children decompensate quickly with minor fluid shifts or electrolyte losses — especially neonates.
🛠️ Anesthetic Strategies by System
🍽️ 1. GERD & Aspiration Risk
- Perform RSI or Modified RSI in:
- Severe GERD
- Neurologically impaired children (CP, shunt patients)
- Obese children
- Known hiatal hernia
Preparation:
- Pre-op fasting confirmed
- Antacid: Sodium citrate or ranitidine
- Metoclopramide optional if delayed gastric emptying
💉 Induction:
- Cricoid pressure (if trained assistant)
- Avoid mask ventilation until intubated
- Cuffed ETT mandatory
- Suction immediately available
🧠 Consider head-up tilt intra-op in severe reflux
💧 2. Renal Disorders (CKD, Dysplasia, Obstruction)
- Risk of hyperkalemia, hypocalcemia, and fluid overload
- Avoid morphine, meperidine, NSAIDs
- Prefer:
- Fentanyl, paracetamol
- Atracurium (organ-independent metabolism)
- Titrate fluids carefully (0.9% NS or RL preferred unless acidotic)
Monitoring:
- ECG if suspecting K⁺ issues
- Check urine output hourly
- Avoid nephrotoxic drugs
- Reduce doses of sedatives, AEDs, and antibiotics
❗ Always clarify: Is this child pre-dialysis? Recently dialyzed? Oliguric?
🍬 3. Diabetes Mellitus & Glucose Disorders
- Check BG before induction, intra-op, and post-op
- Keep glucose between 100–180 mg/dL
- Avoid extremes: hypoglycemia kills quietly, hyperglycemia damages slowly
| Setting | Strategy |
|---|---|
| Elective surgery, well-controlled DM | Skip AM insulin; start 5% Dextrose at maintenance; monitor BG hourly |
| DKA history | Delay surgery until resolved |
| Inborn errors / glycogen storage | Give continuous glucose infusion (D10 or D5NS) |
❗ Avoid Lactate-containing fluids in lactic acidosis or disorders of pyruvate metabolism
💊 4. Steroid-Dependent Children (e.g., CAH, Nephrotic Syndrome)
- If child is on chronic steroids, they need stress dose coverage:
| Situation | Hydrocortisone Dose |
|---|---|
| Minor surgery | 25 mg IV |
| Moderate stress | 50 mg IV |
| Major surgery | 100 mg IV, then 50 mg q6h or infusion |
🧠 Monitor for hypotension, hyponatremia, and hypoglycemia post-op
💡 Additional Tips
- Use Plasmalyte or RL for most major surgeries unless contraindicated
- For fasting >8 hours, always include glucose in maintenance
- If on peritoneal or hemodialysis → reschedule dialysis ideally 24 hrs pre-op
📌 Summary Snapshot Table
| Disorder | Pre-op Concern | Anesthetic Plan | Red Flags |
|---|---|---|---|
| GERD | NPO, reflux? | RSI, antacids | Aspiration |
| CKD | K⁺, fluid status | No morphine/NSAIDs | Acidosis, overload |
| Diabetes | Last insulin? | Monitor BG, D5 infusion | Hypo/hyperglycemia |
| Steroid use | Chronic steroids? | IV hydrocortisone | Adrenal crisis |
| Inborn errors | Fasting? Acidosis? | Dextrose + avoid lactate | Metabolic crash |
🎯 Section E: Other Critical Comorbidities in Pediatric Anesthesia
“Hidden fragilities can tip the balance — stay ahead of them.”
These children often carry less common but high-risk conditions, and many are syndromic or medically complex. Their anesthesia plan must reflect airway anticipation, immunologic caution, and postoperative vulnerability — especially in neurodevelopmental and immunodeficient children.
🧠 1. Neurological & Syndromic Children
🧬 Conditions:
Cerebral palsy, Down syndrome, hydrocephalus, epilepsy, Chiari malformation, myelomeningocele, Pierre Robin, Treacher Collins, achondroplasia.
🧩 Key Considerations
| Issue | Risk | Action |
|---|---|---|
| Difficult airway | Micrognathia, macroglossia, cervical instability | Use video laryngoscope, gentle neck handling |
| Positioning | Contractures, scoliosis | Padding, avoid nerve injury |
| Seizures | Drug interactions | Continue AEDs, avoid enflurane |
| Shunts (VP/VA) | ↑ ICP, vomiting | Avoid hypercarbia, head-up, communicate with neurosurgery |
| GERD, aspiration | Poor tone, delayed gastric emptying | RSI or modified RSI |
| Temperature instability | Poor central control | Warm OR, use warming devices |
| Spasticity | Difficult IV access, contractures | Use EMLA, ultrasound, pre-op plan |
🧠 Down Syndrome: Check for atlantoaxial instability on pre-op records or consider neck precautions if in doubt.
🧪 2. Immunodeficiency & Hematologic Disorders
🔬 Examples:
SCID, HIV, leukemias, aplastic anemia, post-chemo states.
🚨 Anesthetic Concerns
- Sepsis risk: Avoid unnecessary central lines or multiple IV attempts. Use full asepsis.
- Platelet / neutrophil dysfunction: Ask about transfusions, last ANC.
- Delayed wound healing or oxygenation: Optimize peri-op antibiotics and hydration.
💉 If ANC <1000 or Platelets <50k → surgery should be delayed or done with transfusion + antibiotics.
😷 3. Post-COVID Syndrome (MIS-C, chronic fatigue, myocarditis)
📌 Red Flags:
- Residual myocarditis — → do ECG, ECHO if recent hospitalization
- Prolonged fatigue, hypotension, dysautonomia
- Labile BP and HR under anesthesia
- Elevated D-dimer / inflammatory markers → consider coagulopathy risk
🛠️ Strategy:
- Avoid excessive fluids
- Prefer sevoflurane + fentanyl or ketamine in unstable kids
- Monitor blood pressure, EtCO₂, ECG closely
- ICU or HDU stay may be needed after surgery
🌬️ 4. Congenital Airway & Facial Syndromes
👶 Examples:
Laryngomalacia, tracheomalacia, subglottic stenosis, Pierre Robin sequence, Treacher Collins, Goldenhar syndrome
🔧 Tools Ready:
- Nasopharyngeal airway
- Oral airway of various sizes
- Video laryngoscope
- LMA (as rescue in failed intubation)
- ENT backup if known difficult airway
🧠 Consider awake look with mask ventilation to assess ease before committing to full induction in severe deformities.
🧾 Snapshot Table – Other Comorbidities
| Condition | Risk | Must-Do |
|---|---|---|
| Down syndrome | AAI, macroglossia | Neck stability check, difficult airway prep |
| Hydrocephalus | ↑ ICP | Avoid hypercarbia, control BP, head-up |
| CP | Aspiration, spasticity | RSI, careful positioning |
| Immunodeficiency | Sepsis, poor healing | Strict asepsis, avoid unnecessary lines |
| Post-COVID | Myocarditis, coagulopathy | Echo, cautious anesthesia, close monitoring |
| Airway syndromes | Intubation difficulty | Plan for difficult airway, ENT support |
🔚 Pearl to Carry
“Children with rare conditions are often the ones most hurt by general protocols — tailor everything.”
🧠 Document airway difficulty and post-op concerns clearly for next encounter.
📊 Summary Table — Comorbid Child Management Snapshot
| Condition | Pre-op Focus | Induction | Intra-op Red Flag | Post-op Concern |
|---|---|---|---|---|
| TOF | SpO₂, murmur | Ketamine | ↓ SVR → cyanosis | ICU care, oxygenation |
| URTI | Fever, cough | Deep Sevoflurane | Laryngospasm risk | Stridor, PACU observation |
| Cerebral Palsy | Reflux, spasticity | RSI + fentanyl | Difficult IV, abnormal tone | Pain, AED continuation |
| GERD | NPO compliance | RSI | Aspiration risk | Head-up positioning |
| Down Syndrome | Neck flexion check | Propofol + suxamethonium | Difficult mask fit | Apnea, airway obstruction |
| Epilepsy | AED compliance | Propofol | Seizure under stress | Maintain drug levels |
| Obesity / OSA | Airway tone | Short-acting agents | Hypoventilation | PACU monitor, desaturation |
💙 Remember: A syndromic child may have 5 invisible risk factors — one airway, one cardiac, one neurologic, one metabolic, one emotional.
Your job is to find them before they find you.
1️⃣1️⃣ Pediatric Analgesia & Regional Blocks
"Pain Control That Heals — Not Harms"
Effective pain control in children isn’t just about comfort — it’s about recovery, breathing, nutrition, and even neurodevelopment.
This section walks you through a multimodal strategy for pediatric analgesia with safe, practical, and regional options — even in low-resource settings.
🌟 A. Core Principles of Pediatric Analgesia
| Principle | Explanation |
|---|---|
| Multimodal is mandatory | Combine paracetamol, NSAIDs, local blocks, and opioids when needed |
| Dose per kg, not per age | Always base drug doses on accurate weight (daily checked) |
| Opioid-sparing | Use regional blocks and adjuncts to avoid respiratory depression |
| Scheduled > PRN | Regular paracetamol/NSAIDs better than PRN-only approach |
| Pain scales by age | FLACC, Wong-Baker Faces, or NRS depending on age |
💊 B. Safe Drug Options & Dosages
| Drug | Dose | Notes |
|---|---|---|
| Paracetamol | 10–15 mg/kg IV or PO q6h | Max 60 mg/kg/day in neonates |
| Ibuprofen | 5–10 mg/kg PO q6–8h | Avoid in dehydration or renal issues |
| Ketorolac | 0.5 mg/kg IV q6h (max 30 mg) | Potent NSAID; watch for bleeding risk |
| Morphine | 0.05–0.1 mg/kg IV q3–4h | Titrate carefully in neonates/infants |
| Fentanyl | 1–2 mcg/kg IV bolus | Short acting, useful intraop/ICU |
| Tramadol | 1 mg/kg PO/IV q6–8h | Not for <12 yrs or epileptic patients |
| Dexmedetomidine | 0.2–0.5 mcg/kg/h IV | Sedation + analgesia, useful in ICU |
🧠 Avoid codeine — due to variable CYP metabolism in children → risk of respiratory depression or failure to act.
💉 C. Regional Techniques — Practical, Powerful, Proven
1️⃣ Caudal Block
- Indication: Hernia repair, orchidopexy, circumcision, lower limb surgeries
- Dose: Bupivacaine 0.25% or Ropivacaine 0.2%
🔹 0.75–1 ml/kg (max 20 ml) - Additives: Clonidine 1–2 mcg/kg for extended analgesia
🧠 Red Flag: Avoid if sacral dimple, tuft of hair, or spina bifida signs present → rule out tethered cord.
2️⃣ Penile Block
- Indication: Circumcision, hypospadias
- Technique: Dorsal penile nerve block + ring infiltration
- Local: Bupivacaine 0.25% (0.2–0.4 ml/kg)
Tip: Do before incision for preemptive analgesia
3️⃣ Ilioinguinal/Iliohypogastric Block
- Indication: Inguinal hernia, hydrocele
- Approach: Landmark or ultrasound-guided
- Volume: 0.2–0.5 ml/kg of local anesthetic
🧠 Landmark technique sufficient in low-resource settings
4️⃣ TAP Block (Transversus Abdominis Plane)
- Indication: Appendectomy, laparotomy
- Approach: Ultrasound-guided preferred
- Volume: 0.3–0.6 ml/kg per side
🧠 In infants, reduce volume — avoid local anesthetic toxicity!
❤️ D. Special Notes for Tonsillectomy & Hernia Repair
Tonsillectomy:
- Avoid morphine — ↑ risk of OSA-related desaturation
- Use paracetamol + dexamethasone + minimal fentanyl
🔴 Red Flag: Post-tonsillectomy bleeding → full stomach → RSI with suction ready
Hernia Repair:
- Caudal block excellent
- Consider IV paracetamol intra-op
- In preterms: monitor post-op for apnea (especially if <60 weeks post-conceptual age)
🌍 Limited-Resource Strategies
| Problem | Workaround |
|---|---|
| No IV paracetamol | Use suppository or oral suspension |
| No ultrasound for blocks | Use landmark technique for caudal/TAP |
| No dexmedetomidine | Use ketamine infusion in low dose (0.2 mg/kg/h) |
| No clonidine | Slightly increase local anesthetic volume (within safe range) |
📌 Clinical Pearls
- Pain under-treated in children → long-term psychological effects
- Regional anesthesia lowers opioid use and speeds recovery
- Never forget to calculate cumulative local anesthetic dose → avoid LAST (Local Anesthetic Systemic Toxicity)
🧸 1️⃣1️⃣ Parental Counseling & Preoperative Communication
“Easing Fear, Building Trust — One Parent at a Time”
Unlike adults, children don’t give consent — their parents or guardians do. But what they really seek is reassurance, clarity, and trust.
This section equips you to communicate effectively, soothe fears, and build lasting confidence with families in every cultural setting — especially in the Arab world and Iraq.
🗣️ A. The 3 Phases of Communication
| Phase | Focus |
|---|---|
| Pre-op Visit | Explain anesthesia, address concerns, assess child & parent |
| Day of Surgery | Ease separation anxiety, review fasting & meds |
| Post-op | Inform outcome, pain status, any complications |
💬 B. Questions Parents Commonly Ask
| Question | What They’re Really Asking | Suggested Response |
|---|---|---|
| “Will my child wake up?” | Is anesthesia dangerous? | “Yes — we closely monitor every breath and heartbeat.” |
| “Will they feel pain?” | Will they suffer? | “We use special pediatric pain medications and gentle techniques.” |
| “Can I stay with them?” | I’m scared to be separated. | “We’ll keep you informed, and you’ll see them as soon as possible.” |
| “What if something goes wrong?” | Will I lose my child? | “Your child is in skilled hands — every risk is anticipated.” |
🧠 Tip: Answer the emotion behind the question — not just the words.
🧠 C. Explaining Anesthesia in Simple Terms
Use language like:
“We give special sleepy medicine so your child doesn’t feel anything during the procedure. We monitor them every second to keep them safe.”
🪄 Avoid: technical terms like MAC, PEEP, RSI — unless asked.
🎨 Visual aids help: consider a cartoon poster showing the OR and monitor.
🧍 D. Managing Parental Separation Anxiety
Separation may be harder on the parent than the child.
Tips:
- Let one parent escort the child to the OR if policy allows
- Reassure them it’s okay to cry — you stay calm
- Hand-over should be gentle and confident — the anesthesiologist must look composed
📌 In Arab & Iraqi settings, grandparents or uncles may get involved — be respectful but clear who signs consent.
🧕 E. Cultural Considerations in Iraq & Arab Countries
| Cultural Norm | How to Respond Sensitively |
|---|---|
| Large family involvement | Speak to the main guardian, but acknowledge others |
| Distrust of doctors | Offer reassurance through transparency and gentle tone |
| Religious concerns | Respect requests for prayers or verses before induction |
| Language gap | Use Arabic terms when needed (e.g., beynam = sleeping) |
| Modesty concerns | Ensure privacy, especially in adolescent girls |
💡 Involve a pediatrician or nurse if needed to clarify comorbidities, especially in complex cases.
🎁 F. Bonus: Parent–Anesthetist Briefing Box (Visual Insert)
| 🔸 Key Points to Cover Briefly |
|---|
| ✔️ What anesthesia is (safe sleep) |
| ✔️ That your child won’t feel pain |
| ✔️ Who will be present and monitoring |
| ✔️ When they’ll wake up and what to expect |
| ✔️ That you’ll call them as soon as it’s done |
🌈 Closing the Conversation
“We’ll treat your child like one of our own.”
💖 Your tone, posture, and calmness often speak louder than your words.
1️⃣3️⃣ Low-Resource Toolbox
🛠️ Adapting Pediatric Anesthesia in District & Rural Hospitals
In many parts of the world — including our own centers — anesthesiologists face challenges due to limited equipment, outdated drugs, or missing pediatric supplies.
This section is a lifeline: it empowers clinicians to deliver safe pediatric anesthesia even when resources are scarce.
🔧 A. No Sevoflurane? Use Halothane Safely
Halothane, though phased out in high-resource countries, is still widely used across Iraq and other low-income regions.
| Halothane Tips | Details |
|---|---|
| 💉 Slow induction | Use with atropine or glycopyrrolate to prevent bradycardia |
| 🫀 Avoid repeat doses | Risk of myocardial depression and hepatotoxicity |
| 🩺 Monitor HR closely | Reflex bradycardia common in neonates/infants |
| 🔥 Never use with soda lime | Risk of Compound A generation is lower, but caution still needed |
✅ If Halothane is the only inhaled agent: supplement with ketamine or fentanyl for analgesia and to reduce MAC.
🫁 B. No Pediatric Circuits? Modify Adult Circuits
| Problem | Solution |
|---|---|
| Adult circuit too bulky | Use a Mapleson D or Jackson-Rees with low fresh gas flows |
| Heavy mask pull on face | Secure with head straps or improvise with rolled gauze supports |
| No pediatric mask | Use smallest available mask + seal with gauze around edges |
| No pediatric reservoir bag | Use ambu bag’s reservoir, or 500 ml IV bag with valve taping |
🔵 Ensure minimal dead space. A child’s tidal volume is low; adult tubing may lead to CO₂ rebreathing.
🧊 C. Warming Without Bair Hugger
Hypothermia in neonates and infants is dangerous — yet many district hospitals lack warming devices.
Alternatives:
- 🌡️ Warm IV fluids manually in hot water bath (test temperature carefully)
- 🧣 Wrap extremities with cotton wool + plastic to insulate
- 🔥 Use heated water bottles wrapped in towels (never direct contact)
- 🛏️ Foil blankets or plastic wrap for underbody insulation
💡 Pre-warming the OR with a space heater 30 minutes before the case also helps.
🩺 D. Limited Monitoring — What’s the Minimum Safe Setup?
| Ideal | If not available | What to do |
|---|---|---|
| EtCO₂ | Not available | Watch chest rise, RR, retractions, color, and auscultate breath sounds frequently |
| NIBP | Adult cuff too large | Use manual BP with neonatal cuff, or feel pulse pressure by hand |
| SpO₂ | Failing sensor | Use earlobe or palm; reposition every 15–20 mins |
| Temp probe | Not available | Monitor manually — cold hands = cold child |
✅ Always chart clinical signs if monitors are absent: mental status, tone, pulse quality, perfusion.
🩹 E. No Pediatric Doses? Build Dose Cards
Many clinicians fear overdosing due to lack of pediatric calculators.
Build age-based dose cards ahead of time:
| Age | Weight (est.) | Common Doses |
|---|---|---|
| Neonate | 3.5 kg | Ketamine 0.5–1 mg/kg |
| 1 yr | 10 kg | Fentanyl 1–2 mcg/kg |
| 5 yrs | 18–20 kg | Rocuronium 0.6 mg/kg |
🧠 Tape these cards inside your drawer or tray — saves lives.
💬 Cultural Tip
In rural settings, explaining limitations to families calmly builds trust.
Example: “We do not have the newer gas, but we will keep your child completely safe using the protocol that has worked for many years.”
1️⃣4️⃣ Advanced Clinical MCQs — Pediatric Anesthesia
🎯 15 Teaching Questions with Explanations
These questions are crafted to challenge, teach, and reflect real-life pediatric scenarios — perfect for residents, anesthesia techs, and clinicians in training.
🔹 MCQ 1
A 3-year-old child presents for hernia repair. He has a runny nose, occasional cough, and afebrile. On auscultation, mild wheezing is noted. What is the next best step?
A. Proceed with case using deep inhalational induction
B. Cancel case and rebook after 2 weeks
C. Administer salbutamol and proceed with RSI
D. Proceed with ketamine IV induction without premedication
✅ Correct answer: B
🧠 Mild wheezing, even if afebrile, is an LRTI red flag. Elective surgery should be postponed to reduce the risk of laryngospasm and desaturation.
🔹 MCQ 2
Which of the following drugs is most appropriate for induction in a child with Tetralogy of Fallot?
A. Propofol
B. Thiopental
C. Ketamine
D. Midazolam
✅ Correct answer: C
🧠 Ketamine maintains systemic vascular resistance (SVR), reducing right-to-left shunt in TOF. Propofol and thiopental reduce SVR and worsen hypoxia.
🔹 MCQ 3
In a neonate with post-op apnea risk, what monitoring duration is recommended post-anesthesia?
A. 2 hours
B. 4 hours
C. 6–8 hours
D. Overnight or 12–24 hours
✅ Correct answer: D
🧠 Former preterms <60 weeks post-conceptional age require extended monitoring due to apnea risk after anesthesia.
🔹 MCQ 4
You are called to recover a child after tonsillectomy with stridor and increasing retractions. First step?
A. Administer IV midazolam
B. Intubate immediately
C. Give racemic epinephrine via nebulizer
D. Suction and place in lateral position
✅ Correct answer: C
🧠 Post-tonsillectomy stridor = possible airway edema. Racemic epinephrine and oxygen come first. Prepare for intubation if worsening.
🔹 MCQ 5
Estimated weight of a 4-year-old child and appropriate ETT size?
A. 12 kg, 3.5 mm uncuffed
B. 16 kg, 4.5 mm cuffed
C. 18 kg, 5.5 mm cuffed
D. 20 kg, 6.0 mm uncuffed
✅ Correct answer: B
🧠 Weight ≈ (Age × 2) + 8 → (4×2)+8 = 16 kg
ETT size = (Age/4) + 4 → 4.0 + 1 = 5.0 → choose 4.5–5.0 cuffed.
🔹 MCQ 6
Which is the safest inhalational agent in pediatric day-case anesthesia?
A. Desflurane
B. Isoflurane
C. Halothane
D. Sevoflurane
✅ Correct answer: D
🧠 Sevoflurane has rapid onset, smooth induction, and low airway irritation — ideal for children.
🔹 MCQ 7
In a child with cerebral palsy and contractures, key anesthetic concern is:
A. Hypotension
B. Difficult intubation
C. Positioning injury
D. Malignant hyperthermia
✅ Correct answer: C
🧠 CP children often have spasticity, scoliosis, or hip dislocations. Gentle, padded positioning is crucial.
🔹 MCQ 8
Which block is most appropriate for circumcision under sedation without general anesthesia?
A. Caudal
B. TAP
C. Ilioinguinal
D. Penile block
✅ Correct answer: D
🧠 Penile block provides direct analgesia for circumcision. Caudal is more invasive.
🔹 MCQ 9
What is the risk of repeated halothane exposure in children?
A. Seizures
B. Hepatic necrosis
C. Bradycardia
D. Hypoglycemia
✅ Correct answer: B
🧠 Halothane hepatitis is rare but fatal. Avoid repeated exposure within short intervals.
🔹 MCQ 10
Key sign of laryngospasm under anesthesia in a child:
A. Bradycardia
B. No chest movement and silent airway
C. Wheezing and coughing
D. Pink skin and low SpO₂
✅ Correct answer: B
🧠 Tight cord closure leads to no chest rise, no air entry, and silent chest. Immediate treatment is critical.
🔹 MCQ 11
A 5-year-old with asthma requires emergency appendectomy. What is the safest induction agent?
A. Sevoflurane
B. Propofol
C. Ketamine
D. Thiopental
✅ Correct answer: C
🧠 Ketamine is bronchodilatory and ideal in bronchospastic children.
🔹 MCQ 12
A post-tonsillectomy child vomits blood in PACU. What is the immediate step?
A. Suction and observe
B. Give IV ondansetron
C. Re-intubate and secure airway
D. Call ENT to bedside
✅ Correct answer: C
🧠 Post-tonsil bleed = full stomach + airway risk. Re-intubation must be prompt and cautious (RSI preferred).
🔹 MCQ 13
A child with GERD is scheduled for hernia repair. What is the induction of choice?
A. Deep inhalational
B. IV propofol slow
C. RSI with cricoid pressure
D. Ketamine and mask ventilation
✅ Correct answer: C
🧠 GERD = aspiration risk → RSI and cricoid pressure.
🔹 MCQ 14
Which of the following increases MAC in children?
A. Hyperthermia
B. Hypoxia
C. Anemia
D. Prematurity
✅ Correct answer: A
🧠 MAC ↑ with hyperthermia, chronic stimulant use, red hair. ↓ with hypothermia, anemia, and elderly age.
🔹 MCQ 15
You are called to help insert IV in a 6-month-old dehydrated child. Best site?
A. Foot dorsal vein
B. External jugular
C. Intraosseous
D. Femoral vein
✅ Correct answer: C
🧠 Intraosseous access is safe, fast, and lifesaving in pediatric shock if IV fails.
1️⃣5️⃣ Summary Tables & Quick Reference
📊 “Pediatric Anesthesia at a Glance” Poster + Printables
This section is designed for real-time OR use — screenshots for your phone, printouts for hospital walls, and quick-reference flashcards for your anesthesia trolley.
📌 A. Normal Pediatric Vitals by Age
| Age | HR (bpm) | RR (breaths/min) | SBP (mmHg) | SpO₂ |
|---|---|---|---|---|
| Neonate | 100–160 | 30–60 | 60–90 | >94% |
| Infant (1–12 mo) | 100–160 | 30–50 | 70–100 | >94% |
| Toddler (1–3 yrs) | 90–150 | 24–40 | 80–100 | >94% |
| Preschool (4–5 yrs) | 80–140 | 22–34 | 80–110 | >94% |
| School Age (6–12 yrs) | 70–120 | 18–30 | 90–120 | >94% |
| Adolescent | 60–100 | 12–20 | 90–130 | >94% |
🧮 B. Endotracheal Tube Size & Depth
| Age | Formula | ETT Size (cuffed) | ETT Depth (cm) |
|---|---|---|---|
| <1 yr | Neonatal charts | 3.0–3.5 | Weight-based |
| 1–10 yrs | (Age ÷ 4) + 3.5 | e.g. 4.5–5.0 | (ETT size × 3) |
| >10 yrs | Adult sizing | 6.0–7.0 | Confirm by auscultation |
🧠 Always confirm with auscultation + EtCO₂. Leak test at 20–25 cmH₂O is ideal.
💊 C. Drug Dose Essentials
| Drug | Dose | Route |
|---|---|---|
| Propofol | 2–3 mg/kg | IV |
| Ketamine | 1–2 mg/kg | IV / 4–6 IM |
| Fentanyl | 1–2 mcg/kg | IV |
| Midazolam | 0.05–0.1 mg/kg | IV/IM/PO |
| Atropine | 10–20 mcg/kg | IV |
| Glycopyrrolate | 5–10 mcg/kg | IV |
| Rocuronium | 0.6–1.2 mg/kg | IV |
| Succinylcholine | 1–2 mg/kg | IV |
| Paracetamol | 15 mg/kg | PO/PR |
| Ibuprofen | 10 mg/kg | PO |
🧠 Use diluted doses for infants and double-check decimal points carefully.
🎯 D. Pediatric Anesthesia Snapshot: “One Glance” Poster
| Domain | Snapshot |
|---|---|
| Weight Estimate | (Age × 2) + 8 |
| ETT Size | (Age ÷ 4) + 3.5 |
| ETT Depth | (Size × 3) |
| Fluids (4-2-1 Rule) | 4 ml/kg/hr for 1st 10 kg, 2 ml/kg/hr next 10 kg, then 1 ml/kg/hr |
| Maintenance | 100/50/20 rule = ml/kg/day |
| Blood Volume | Neonate: 90 ml/kg, Infant: 80 ml/kg, Child: 70 ml/kg |
| Acceptable Blood Loss | [EBV × (Hct_i - Hct_f)] ÷ Hct_i |
📸 We will prepare this as a downloadable PDF or phone wallpaper if you’d like.
📎 Optional Printable Tools
- ✅ ETT size & drug quick-card
- ✅ Pediatric fluid cheat sheet (include 22/17 formula)
- ✅ Regional block reference
- ✅ Post-extubation monitoring checklist
🔟 Final Words
Pediatric anesthesia is a delicate balance of physiology, trust, and precision.
It’s not just about delivering medication — it’s about holding a family’s hope with steady hands.
This Mastery Guide was built to give you the tools to act safely, confidently, and compassionately — from district hospitals in Wasit to advanced centers worldwide.
Whether you're preparing for a tonsillectomy or a neonate with complex heart disease, remember:
Structure replaces chaos. Vigilance prevents tragedy. Compassion completes your skill.
This guide is your reference when managing pediatric anesthesia — in every setting.
Stay structured. Stay vigilant. Act wisely. 🧠
📌 Prepared for Dr. Amir Fadhel – Specialist in Anesthesiology and Critical Care
📅 Created: 05/06/2025
📅 Last Updated: 07/06/2025
🔗 Explore the full collection: Mastery Series in Anesthesia & Critical Care