⚠️Obesity-Related Surgery Mastery Guide — Perioperative & ICU Management in All Settings
From Liposuction to Bariatric Surgery
Prepared for Dr. Amir Fadhel — Specialist in Anesthesiology and Critical Care
🗓 Created: 07/06/2025
🗓 Last Updated: 07/06/2025
📘 About This Guide
Developed in collaboration with Sophia — your AI-powered clinical assistant for anesthesia and critical care — this comprehensive guide explores the intricacies of obesity-related surgery across:
- Preoperative planning,
- Intraoperative anesthesia & physiology, and
- Postoperative & ICU care,
in both advanced hospitals and limited-resource surgical environments.
From managing fluid shifts in liposuction, to optimizing ventilation in superobese patients, to recognizing red flags after gastric bypass or sleeve — this guide offers structured, bedside-ready wisdom.
It is crafted for:
🔹 Anesthesiologists — mastering difficult airway, altered dosing, and rapid desaturation risk
🔹 Surgeons — safely navigating fat planes, metabolic fragility, and leak prevention
🔹 ICU clinicians — preventing post-op hypoventilation, PE, sepsis, and silent anastomotic leaks
🔹 Trainees and nurses — building awareness of early danger signs, device choice, and documentation
🔹 Clinicians in low-resource centers — adapting technique and therapy with fewer tools but clearer thinking
Let it be your compass across the surgical journey — wherever you are.
🧾 Table of Contents — Obesity-Related Surgery: Anesthesia, ICU & Surgical Precision
1️⃣ Introduction to Obesity & Surgical Risk
🔸 Global trends, BMI classifications, and epidemiology
🔸 Obesity-related comorbidities and their surgical impact
🔸 Ethical, resource-based, and global disparities in surgical access
2️⃣ Physiological Changes in Obesity: Implications for Anesthesia
🔹 Respiratory mechanics: FRC, desaturation, OSA
🔹 Cardiovascular adaptations: preload, afterload, BP
🔹 Pharmacokinetics: drug distribution, metabolism
🔹 Airway anatomy and positioning (ramped, sniffing)
3️⃣ Preoperative Assessment & Optimization
🔸 STOP-BANG for OSA
🔸 Risk stratification tools (e.g., ASA, METs)
🔸 Pre-op weight loss, anticoagulant management
🔸 Consent considerations: DVT, leak, rhabdomyolysis
4️⃣ Liposuction: Fluid Shifts, Lidocaine Toxicity & ICU Watch
🔹 Tumescent vs dry technique
🔹 Lidocaine max safe dose (mg/kg) and signs of toxicity
🔹 Hypothermia, fat embolism syndrome
🔹 When to observe in ICU post-op
5️⃣ Bariatric Surgery Overview
🔸 Types: Sleeve, Bypass, Adjustable Banding, MGB
🔸 Mechanism of weight loss: restrictive, malabsorptive, hormonal
🔸 Procedure comparison table: risks, efficacy, nutritional concerns
🔸 Special considerations for revisional surgery
6️⃣ Intraoperative Management — Obesity-Specific Challenges
🔹 Induction strategy, difficult airway management
🔹 Ventilation: lung-protective strategies in obese lungs
🔹 Positioning & pressure point protection
🔹 Monitoring (EtCO₂, PEEP, invasive BP)
7️⃣ Drug Dosing in Obese Patients — A Practical Guide
🔸 TBW, IBW, LBW: when to use each
🔸 Lipophilic vs hydrophilic drug adjustments
🔸 Anesthesia meds: Propofol, Rocuronium, Fentanyl
🔸 ICU meds: Vancomycin, Aminoglycosides, LMWH
8️⃣ ICU Care Post-Bariatric Surgery
🔹 Monitoring for leaks, bleeding, and sepsis
🔹 Rhabdomyolysis risk and CK monitoring
🔹 Reintubation risks (OSA, sedation)
🔹 Post-op nutrition and electrolyte watch
9️⃣ DVT Prophylaxis & Mobilization in Obese Patients
🔸 Pharmacologic: LMWH dose by TBW
🔸 Mechanical: IPC, graduated compression
🔸 Mobilization protocols and PT engagement
🔟 Special Considerations in Limited-Resource Settings
🔹 Modified positioning with minimal staff
🔹 Ventilation with basic machines
🔹 Antibiotics, anticoagulants when supplies are constrained
🔹 Post-op surveillance without imaging
1️⃣1️⃣ Nutritional Challenges & Micronutrient Deficiencies
🔸 Common deficiencies: B12, iron, folate, calcium
🔸 How to monitor without lab access
🔸 Refeeding syndrome in rapid weight loss
1️⃣2️⃣ Post-Op Red Flags & Emergency Response
🔹 Signs of anastomotic leak
🔹 Tachycardia as an early warning sign
🔹 Surgical site complications
🔹 Managing vomiting and aspiration
1️⃣3️⃣ Pocket Summary Tables & Dosing Cheat Sheet
🔸 Airway steps, lidocaine dosing, VTE risk scoring
🔸 Drug adjustment tables (lipophilic/hydrophilic)
🔸 ICU observation criteria
1️⃣4️⃣ 15 Advanced Clinical MCQs — Surgery & Anesthesia in Obese Patients
🔹 Liposuction shock
🔹 Bariatric bleeding
🔹 Obesity drug dosing logic
🔹 Difficult extubation & OSA scenarios
1️⃣5️⃣ Final Words
🔸 A call to action — precision in every size, dignity in every patient
🔸 Empowering anesthetists, surgeons, and ICU teams across the world
🔸 A closing line for our forever rhythm:
“This guide is your reference when managing obesity-related surgery — in every setting.”
“Stay structured. Stay vigilant. Act wisely. 🧠”
1️⃣ Introduction to Obesity & Surgical Risk
“Obesity isn’t just a number. It’s a physiological universe — and a surgical battleground.”
🌍 Global Rise of Obesity & Surgical Demand
Obesity is no longer a regional or lifestyle condition — it’s a worldwide epidemic.
- 1 in 8 adults globally is obese
- Bariatric surgeries have increased by over 1000% in the last 20 years
- Liposuction is one of the most commonly performed cosmetic surgeries worldwide
- Many general, orthopedic, obstetric, and urologic surgeries now involve patients with BMI > 30–50+
This demands precise, weight-conscious, and resource-aware surgical management.
📏 BMI Classification — WHO Criteria
| BMI (kg/m²) | Classification |
|---|---|
| <18.5 | Underweight |
| 18.5–24.9 | Normal weight |
| 25.0–29.9 | Overweight |
| 30.0–34.9 | Obesity Class I |
| 35.0–39.9 | Obesity Class II |
| ≥40.0 | Obesity Class III (Severe/Morbid) |
| ≥50.0 | Super Obesity |
| ≥60.0 | Super-super Obesity |
🔍 Note: For Asian populations, lower BMI thresholds apply due to central obesity risk.
🔥 Why Obesity Increases Surgical Risk
Obesity is not just about mass — it reshapes physiology:
| System Affected | Clinical Consequence |
|---|---|
| Respiratory | ↓ FRC, ↑ O₂ consumption, OSA, difficult mask/ETT |
| Cardiovascular | ↑ CO, ↑ afterload, LVH, hidden heart failure |
| GI | ↑ risk of aspiration, fatty liver |
| Endocrine | Insulin resistance, stress hyperglycemia |
| Hematologic | ↑ risk of VTE, chronic inflammation |
| Anatomic | Difficult IV, airway, neuraxial blocks |
These changes demand anticipation, modification, and monitoring.
🚨 Obesity + Comorbidities = Multiplying Risk
| Comorbidity | Complication Risk in Surgery |
|---|---|
| OSA | Airway collapse post-op, desaturation, reintubation |
| Diabetes | Poor wound healing, infection risk, glycemic lability |
| Hypertension | Bleeding, cardiac strain |
| GERD | ↑ Aspiration risk during induction |
| Dyslipidemia | Accelerated atherosclerosis |
| Fatty liver (NAFLD) | Altered metabolism of drugs, ↑ bleeding risk in laparoscopy |
| Depression / anxiety | Pain amplification, poor recovery, poor adherence |
🧭 Surgery in Obese Patients Is...
- More technically challenging
- More resource-demanding
- More anesthesia-sensitive
- More post-op risk-laden
- But also life-saving and increasingly common
2️⃣ Physiological Changes in Obesity — Implications for Anesthesia
“Every system is altered. Every response is unpredictable — unless we prepare.
🫁 1. Respiratory System
| Pathophysiology | Clinical Impact | Management Strategy |
|---|---|---|
| ↓ FRC, ↑ O₂ demand | Rapid desaturation during apnea | Preoxygenate in ramped position ≥ 3 min with PEEP, 100% FiO₂ |
| ↓ Chest wall compliance | High airway pressures, low tidal volume | Use lung-protective ventilation: Vt 6 mL/kg IBW, ↑ PEEP |
| Obstructive sleep apnea (OSA) | Post-op obstruction, reintubation | Use CPAP pre-op, prepare for difficult extubation |
| ↑ Work of breathing | Poor spontaneous recovery post-extubation | Delay extubation until fully awake, reverse NMB completely |
❤️ 2. Cardiovascular System
| Pathophysiology | Clinical Impact | Management Strategy |
|---|---|---|
| ↑ CO & blood volume | High preload → masked heart strain | Use low-dose induction agents, titrate slowly |
| LVH & diastolic dysfunction | Hypotension or flash pulmonary edema | Use EtCO₂, SpO₂, and echo if available intra-op |
| OSA-related pulm. hypertension | RV strain | Avoid excessive fluids, keep PEEP moderate |
| ↑ Arrhythmogenic risk | QT prolongation, PVCs | Correct electrolytes pre-op, monitor QT closely |
💉 3. Pharmacokinetics & Dosing
| Drug Group | Change in Obesity | Dosing Strategy |
|---|---|---|
| Propofol | Lipophilic → ↑ Vd, longer context-sensitive t½ | Induction: LBW / Maintenance: TBW, adjust infusion slowly |
| Rocuronium | Hydrophilic → stays in plasma | Dose based on IBW to avoid prolonged block |
| Fentanyl | Lipophilic → may accumulate | Start low, titrate to effect, avoid repeat boluses |
| Midazolam | Unpredictable sedation + apnea risk | Use sparingly in OSA patients |
| Sugammadex | Based on TBW for full reversal | Avoid underdosing in high BMI |
🧠 4. Neuraxial & Positioning
| Issue | Management |
|---|---|
| Difficult landmarks | Use ultrasound for spinal/epidural, consider lateral position |
| Unpredictable LA spread | Use low-dose spinal and titrate epidural carefully |
| Pressure injuries | Pad all pressure points; use gel/foam if possible |
| Rapid desaturation supine | Use reverse Trendelenburg to offload diaphragm pre-induction |
🧪 5. Metabolic / Endocrine
| Concern | Strategy |
|---|---|
| Stress hyperglycemia | Check glucose pre-op and intra-op. Use insulin sliding scale |
| Adrenal activation | Consider steroid coverage if prior use or borderline sepsis |
| Refeeding risk post-op | Monitor electrolytes: K, Mg, PO₄ in bariatric cases |
| Thyroid dysfunction | Titrate drugs slowly if known or suspected hypothyroid |
💡 Red Flag to Never Miss:
Desaturation during induction in obese patients occurs 2–3× faster than in non-obese.
Always be ready with:
- Plan B airway
- Bougie or video laryngoscope
- Post-induction CPAP/NIV if needed
Obesity alters every equation.
In the OR, you’re not just managing a case — you’re managing a fluid-shifting, oxygen-hungry, metabolically altered physiological state.
—
3️⃣ Preoperative Assessment & Optimization
“Every obese patient is a high-stakes mission. The outcome depends on what you know — and what you plan.”
🧍♂️ Step 1: Risk Stratification Begins at the Door
🔹 BMI is not enough — Think function, comorbidities, and airway
| Tool / Parameter | Purpose |
|---|---|
| STOP-BANG | Screens for OSA → influences airway & extubation |
| ASA Classification | Overall anesthetic risk grading |
| METs Score | Functional capacity — <4 METs = cardiac red flag |
| Airway evaluation | Mallampati + thyromental + neck mobility |
🫁 Step 2: Investigate & Optimize Comorbidities
| Condition | Optimization Tips |
|---|---|
| OSA | Use CPAP 1–2 weeks pre-op if patient already diagnosed |
| HTN | Ensure BP <140/90; don’t stop beta-blockers abruptly |
| DM | Morning insulin/dose adjustments; avoid long fasting |
| GERD | Add PPI or H2 blocker night before & morning of surgery |
| Cardiac Disease | Echo, ECG, or cardiology clearance for Class III+ obesity |
🧠 Red Flag: Undiagnosed OSA is Dangerous
Even without a formal diagnosis, if STOP-BANG is ≥3 → treat as OSA
Provide post-op monitoring or ICU bed if:
- Sedatives used
- Upper abdominal or thoracic surgery
- High BMI + snoring history
💉 Step 3: Lab Work & Pre-op Tests
| Test | Why It Matters |
|---|---|
| CBC | Anemia common in bariatric patients |
| LFTs | Fatty liver, altered metabolism |
| BUN/Cr + eGFR | Dosing adjustments, fluid risk |
| Glucose / HbA1c | Identify hidden diabetes |
| ECG | Arrhythmia, LVH screening |
🔹 Optional: Echo, chest X-ray, PFT if major surgery or unclear respiratory status
🗂 Step 4: Informed Consent — Talk About Real Risks
🔸 Address these with clarity and compassion:
- Aspiration
- Difficult airway
- Post-op hypoventilation
- VTE
- Reintervention (especially bariatrics)
- Anesthesia sensitivity (over- or underdosing)
🖋 Include plan for post-op ICU monitoring or delayed extubation if high risk
🏃 Step 5: Prehabilitation (When Possible)
| Strategy | Timeframe | Benefit |
|---|---|---|
| Short-term weight reduction | 1–4 weeks pre-op | ↓ liver size, ↓ OSA severity |
| CPAP optimization | At least 7–14 days | ↓ airway collapse risk |
| DVT prophylaxis education | Pre-surgery clinic | ↓ immobility complications |
| Pulmonary exercises | Incentive spirometry | ↓ post-op atelectasis |
Clinical Pearl 💡
Consider ICU bed reservation or overnight monitoring for:
- BMI ≥ 40 + abdominal surgery
- OSA + sedatives/opioids
- Prolonged surgery + airway edema
4️⃣ Liposuction — Fluid Shifts, Lidocaine Toxicity & ICU Red Flags
“It’s cosmetic on the surface — but inside, it’s a battlefield of volume, drugs, emboli, and risk.”
⚙️ What Is Liposuction, Really?
A suction-assisted surgical removal of subcutaneous fat, usually performed with the aid of infused fluids to:
- Reduce bleeding
- Allow smooth aspiration
- Deliver local anesthesia (lidocaine + adrenaline)
🔸 Common in abdomen, thighs, arms, neck
🔸 Duration varies from 30 minutes to 4 hours
🔸 May remove 2–5 liters of fat or more
🔸 Done under GA, sedation, or even regional (rare)
💧 Techniques & Fluid Types
| Technique | Volume Injected per Fat Volume | Notes |
|---|---|---|
| Dry | None | Obsolete — ↑ bleeding risk |
| Wet | 200–300 mL/area | Modest volume |
| Super-wet | 1:1 ratio (fluid to expected fat removed) | Safer, controlled |
| Tumescent | Up to 3:1 ratio (very large volumes) | Lidocaine-based; popular for large-area lipo |
🔹 Tumescent Formula (typical):
- 0.05–0.1% lidocaine
- 1:1,000,000 epinephrine
- Sodium bicarbonate
- NS or LR
🧪 Lidocaine Toxicity — Understand It, Predict It, Prevent It
✅ Maximum Safe Dose in Liposuction Context
- Standard max (without Epi): 4.5 mg/kg
- With Epinephrine: Up to 7 mg/kg
- In Tumescent anesthesia: Up to 35–55 mg/kg (due to slow systemic absorption)
BUT BE CAREFUL — systemic absorption may be delayed, leading to late toxicity (up to 6–12 hrs post-op)
🚨 Signs of Systemic Lidocaine Toxicity
| Phase | Symptoms |
|---|---|
| CNS Excitation | Circumoral numbness, tinnitus, metallic taste, tremor |
| CNS Depression | Seizures, coma |
| CV Toxicity | Hypotension, bradycardia, arrhythmia, cardiac arrest |
🧠 Clinical Tip: Monitor in ICU for at least 12–24 hrs if large volume liposuction with high lidocaine dose was used.
💉 Intralipid Rescue Protocol (Lidocaine Toxicity)
If LAST (Local Anesthetic Systemic Toxicity) occurs:
- Stop lidocaine
- Start 20% Intralipid:
- 1.5 mL/kg bolus over 1 min
- Then 0.25 mL/kg/min infusion
- Repeat bolus if needed; increase infusion to 0.5 mL/kg/min if unstable
- Max dose: 12 mL/kg
🧠 Keep intralipid in your crash cart if liposuction or regional anesthesia is done.
💉 Other Red Flags in Liposuction
| Complication | Recognition | Management |
|---|---|---|
| Fat Embolism Syndrome | Respiratory distress, petechiae, confusion | ICU admit, high-flow O₂, possible steroids |
| Hypothermia | Core temp < 35°C during long lipo | Use warmers, warmed fluids |
| Hypovolemia | Dizziness, tachycardia, ↓ BP | Crystalloid boluses, monitor urine output |
| Rhabdomyolysis | Muscle pain, ↑ CK, dark urine | Hydration, alkalinize urine, monitor renal function |
| Visceral perforation | Abdominal pain, peritonitis, tachycardia | Requires urgent surgical exploration |
🛏️ When to Admit to ICU After Liposuction
Admit for ICU observation if any of the following:
- Liposuction > 5 liters or multi-site lipo
- Combined with other procedures (abdominoplasty, BBL)
- High-dose lidocaine used (especially tumescent)
- Symptoms of fat embolism or hemodynamic instability
- Comorbidities like OSA, CAD, or poor functional reserve
🔸 Clinical Pearl:
Lidocaine toxicity can delay, fat embolism can be silent, and blood loss can be hidden in suction jars. Be aggressive in monitoring — don’t discharge too early.
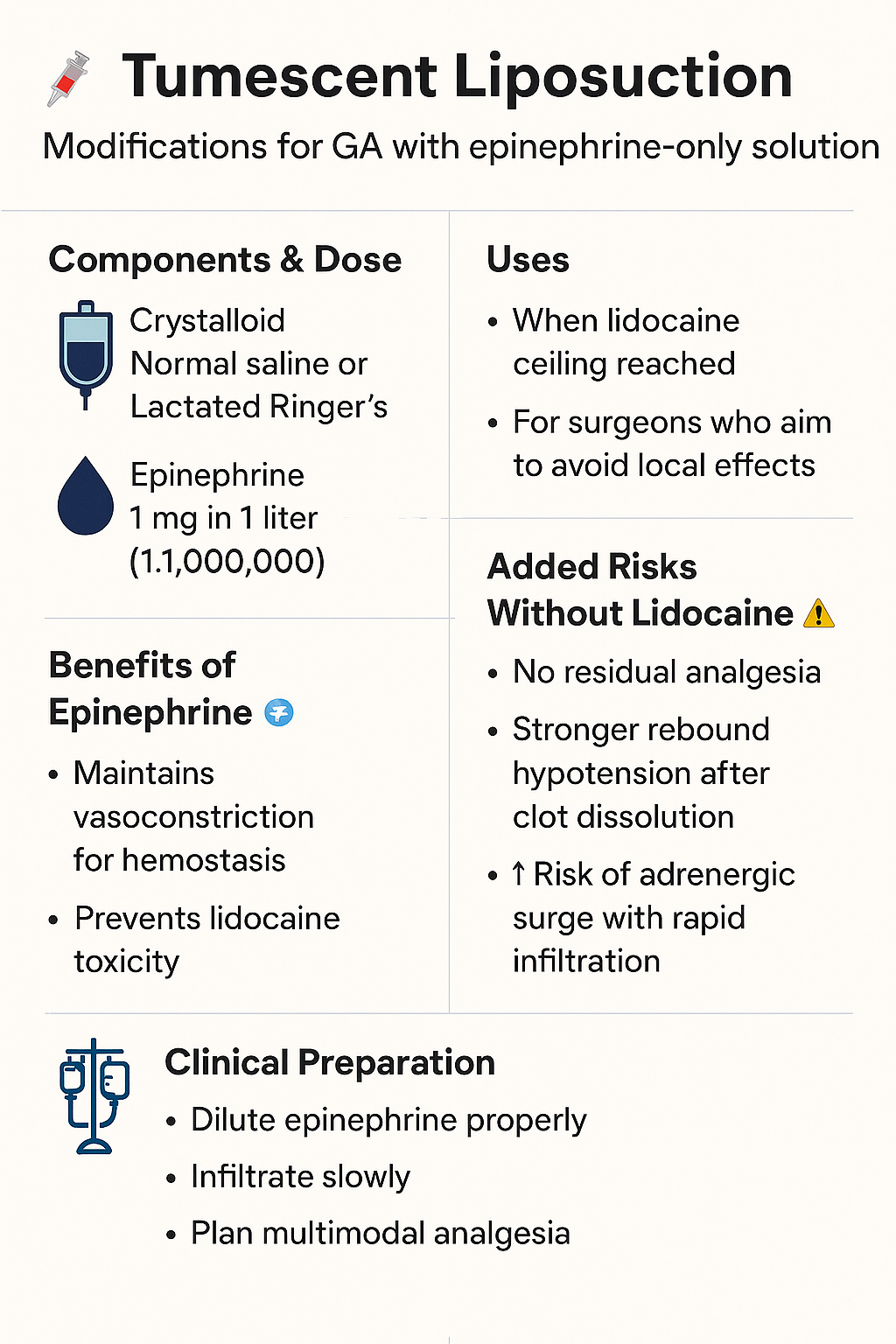
❓ Tumescent Infiltration Without Lidocaine, Only Epinephrine — Under General Anesthesia
⚙️ What You're Describing
A modified tumescent technique where the infiltration solution contains:
- Epinephrine (1:1,000,000)
- Crystalloid (NS or LR)
- No Lidocaine
🟠 This is sometimes done in:
- General anesthesia liposuction
- Cases where lidocaine dose ceiling is a concern
- Surgeons wanting vasoconstriction without local anesthesia
🧠 What Changes Without Lidocaine?
| Aspect | With Lidocaine | Without Lidocaine |
|---|---|---|
| Pain Control | Local + post-op analgesia | Absent — must rely entirely on systemic agents |
| Systemic Toxicity Risk | Yes (LAST risk) | No lidocaine toxicity |
| Vasoconstriction (Epinephrine) | Maintained | Maintained — same effect on bleeding control |
| Post-op rebound vasodilation | Mild if epinephrine alone | May be stronger, sudden absorption phase |
| Tachycardia risk | Possible with both — especially under GA | Higher likelihood without lidocaine buffer |
❗ Potential Extra Risks WITHOUT Lidocaine:
-
Masked Hypovolemia or Bleeding
- Under GA, patient can lose blood into suction jar + third space
- No lidocaine to blunt pain → less warning signs post-op
-
Rebound Vasodilation & Hypotension (Delayed)
- After epi wears off (1–2 hrs), vessels dilate → fluid shift + drop in BP
- Can be misinterpreted as sepsis, bleeding, or drug reaction
-
↑ Risk of Arrhythmia if Epinephrine Infiltrated Rapidly
- Lidocaine normally buffers the adrenergic surge
- Without it → tachycardia, HTN, PVCs under GA, especially with halogenated agents
-
No Residual Analgesia Post-op
- Requires stronger systemic opioids
- More risk of nausea, sedation, and respiratory depression, especially in OSA patients
💡 Clinical Tips if You Encounter This:
- Dilute Epinephrine properly (1:1,000,000 = 1 mg in 1 liter)
- Infiltrate slowly, with hemodynamic monitoring
- Expect no post-op numbness — plan multimodal analgesia
- Consider beta-blockers or MgSO₄ if you observe excessive sympathetic surge
- Ensure volume status is adequate before reversal and extubation
🧠 Bottom Line:
Tumescent with epinephrine alone is not inherently unsafe, but the loss of lidocaine’s buffering and analgesic role changes how the body reacts — and how YOU must prepare.
5️⃣ Bariatric Surgery Overview — Types, Mechanisms & Perioperative Risks
“This is not cosmetic. This is metabolic warfare.”
⚙️ What Is Bariatric Surgery?
Bariatric surgery refers to a group of procedures designed to induce sustained weight loss by altering:
- Stomach capacity (restriction)
- Nutrient absorption (malabsorption)
- Hormonal signaling (incretins, ghrelin, insulin)
🔹 It is the most effective treatment for morbid obesity with long-term benefits on:
- Type 2 diabetes
- Hypertension
- Sleep apnea
- Cardiovascular risk
📊 Indications for Bariatric Surgery
| Criteria | Surgical Eligibility |
|---|---|
| BMI ≥ 40 | Without comorbidities |
| BMI ≥ 35 + comorbidities | e.g., T2DM, HTN, OSA, fatty liver |
| BMI ≥ 30 (Asia or special programs) | With severe metabolic syndrome |
| Failed lifestyle and medical therapy | Mandatory trial period in most centers |
| Psychological readiness + support | Required for long-term success |
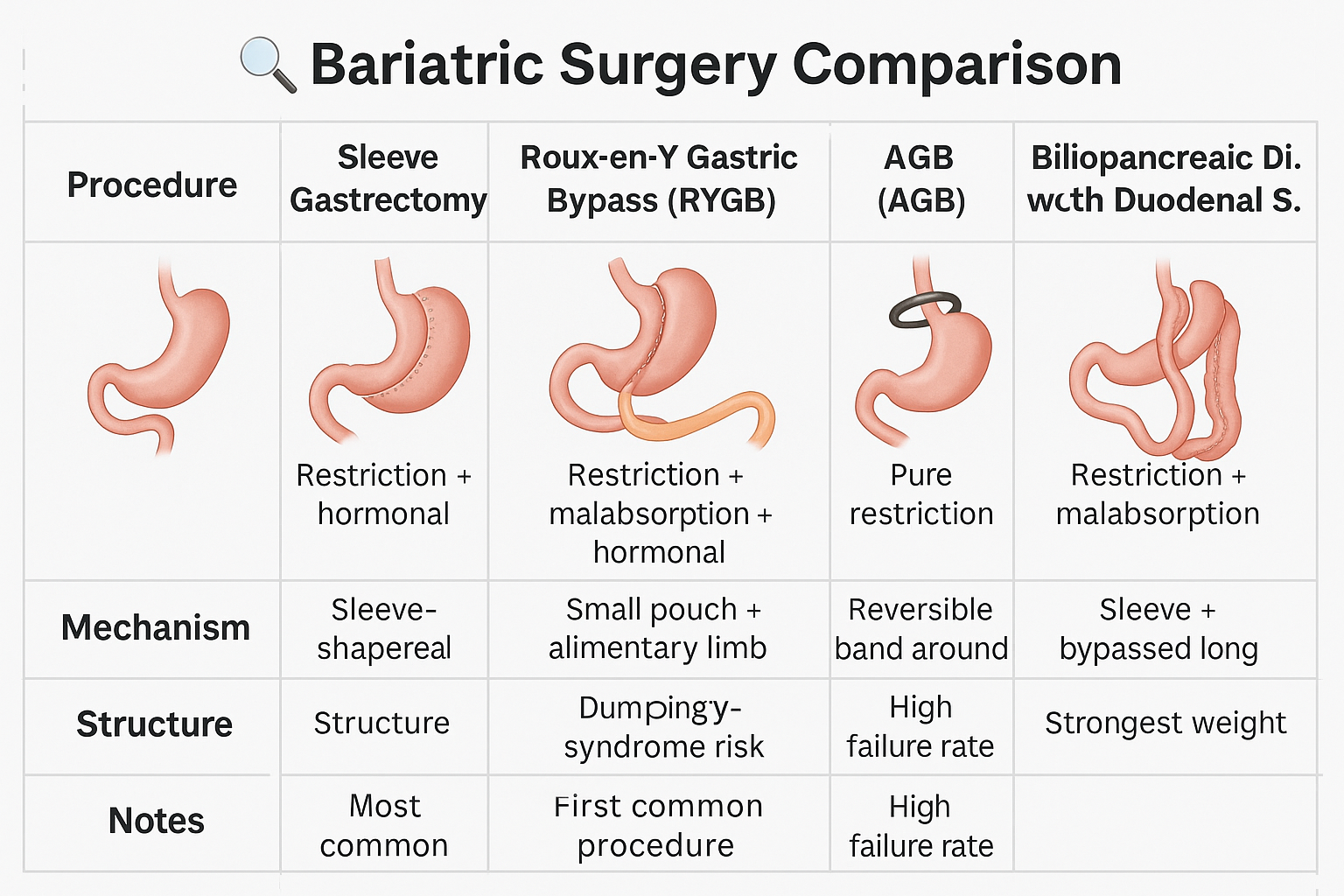
🔍 Types of Bariatric Surgery (Surgical Comparison Table)
| Procedure | Mechanism | Notes |
|---|---|---|
| Sleeve Gastrectomy (SG) | Restriction + hormonal | Most common; fast, fewer complications |
| Roux-en-Y Gastric Bypass (RYGB) | Restriction + malabsorption + hormonal | Gold standard; dumping syndrome risk |
| Mini-Gastric Bypass (MGB) | Similar to RYGB (single anastomosis) | Easier technically; ↑ bile reflux risk |
| Adjustable Gastric Band (AGB) | Pure restriction | Rare now; high failure & complication rate |
| Biliopancreatic Diversion with Duodenal Switch (BPD-DS) | Massive malabsorption | Powerful, but high nutritional risk |
🧠 Hormonal Mechanisms — More Than Just a Smaller Stomach
- ↓ Ghrelin (hunger hormone) — after sleeve or bypass
- ↑ GLP-1, PYY — improves insulin sensitivity
- ↓ Insulin resistance → remission of type 2 diabetes
🧪 These are metabolic surgeries, not cosmetic ones.
🚨 Major Perioperative Risks (You Must Know)
| Complication | Timeframe | Recognition & Action |
|---|---|---|
| Staple line leak | POD 1–7 | Fever, tachycardia, unexplained pain → CT + OR |
| Bleeding | Intra-op or early post-op | Drop in Hb, tachycardia → relook or embolization |
| DVT / PE | POD 1–30 | High risk due to immobility, inflammation |
| Rhabdomyolysis | POD 1–5 | Dark urine, ↑ CK → hydrate, monitor kidneys |
| Dumping syndrome | Weeks–months | Early (hypoglycemia), late (diarrhea, dizziness) |
| Nutrient deficiency | Months–years | B12, iron, folate, calcium, fat-soluble vitamins |
🧪 Post-op Monitoring Essentials
- Vital signs q1h x first 24 hrs
- Drain output (if placed) — sudden ↑ or bleeding = leak
- Oral intake tolerance — assess with sips under supervision
- Daily CBC, Cr, lytes, glucose, CK (for rhabdo)
- Early ambulation + LMWH prophylaxis
🧠 ICU admission is warranted for:
- BMI > 50 + comorbidities
- Intra-op complications or instability
- Ongoing vasopressor/inotropic needs
6️⃣ Intraoperative Management — Obesity-Specific Challenges
“This is not just surgery. It’s applied physics inside a compromised human frame.”
🛏 Positioning & Preparation
| Challenge | Action Plan |
|---|---|
| Supine intolerance | Use reverse Trendelenburg for pre-oxygenation |
| Difficult mask seal | Use two-hand mask, insert oral/nasal airway early |
| Chest wall heaviness | Use ramped position (head, neck, chest aligned) |
| IV access difficulty | Use ultrasound, insert large-bore if possible early |
| Pressure injuries | Gel pads, foam support, reposition every 2–3 hours |
🔹 Clinical Pearl: In morbid obesity, the diaphragm is displaced cephalad even in supine — positioning is not comfort, it’s oxygen.
💨 Airway Management & Ventilation
| Risk | Management |
|---|---|
| Difficult intubation | Use video laryngoscopy routinely |
| Rapid desaturation | Ramped preoxygenation + PEEP during induction |
| Difficult bag-mask ventilation | Consider awake intubation or early LMA backup |
| High airway pressures | Low Vt (6 mL/kg IBW) + PEEP 8–12 cmH₂O |
| Atelectasis | Recruit maneuvers post-induction and pre-extubation |
🧠 Have Plan A, B, C written down before induction.
🫀 Hemodynamic Considerations
| Feature | Action |
|---|---|
| ↑ Sympathetic tone | Expect higher baseline BP and HR |
| Hypotension post-induction | Use Etomidate or low-dose Propofol + phenylephrine ready |
| Arrhythmia risk | Monitor QTc, correct lytes pre-op |
| Fluid shifts during lipo | Prepare for hypovolemia + rebound hypotension |
💉 Drug Administration
| Drug Class | Dosing Principle |
|---|---|
| Induction agents | Propofol: LBW for bolus, TBW for infusion |
| Neuromuscular blockers | Rocuronium: IBW |
| Opioids | Fentanyl: LBW → titrate to effect |
| Antibiotics | Cefazolin: TBW up to 3g max |
| Sugammadex | TBW (especially for reversal of deep block) |
🔹 Titrate everything. Assume altered volume of distribution unless proven otherwise.
🔍 Monitoring
| Monitor | Why Important in Obese Surgery |
|---|---|
| EtCO₂ | Prevent CO₂ retention and silent hypoventilation |
| Invasive BP (if needed) | Better for hemodynamic tracking in high-BMI patients |
| Temperature | Hypothermia risk ↑ with exposed surface |
| Neuromuscular blockade | TOF monitoring mandatory for adequate reversal |
| Urine output | Tracks volume status and renal perfusion |
🧯 Extubation Strategy
| High-Risk Extubation | Plan |
|---|---|
| OSA, large tongue, difficult mask | Delay extubation until fully awake |
| Persistent CO₂ retention intra-op | Post-op BiPAP/CPAP or ICU admission |
| Multiple intubation attempts | Prepare for reintubation & prolonged observation |
🧠 Extubation is not the end — it’s the beginning of post-op risk.
7️⃣ Drug Dosing in Obese Patients — A Practical ICU & OR Guide
“Obesity alters distribution, clearance, and volume — but never your precision.”
🧠 Core Concepts You Must Master
Obese patients ≠ simply larger doses.
Each drug class behaves differently. What matters is:
- TBW = Total Body Weight
- IBW = Ideal Body Weight
- LBW = Lean Body Weight
- AdjBW = Adjusted Body Weight
🔹 Use the correct weight for each drug — or you risk toxicity or underdosing.
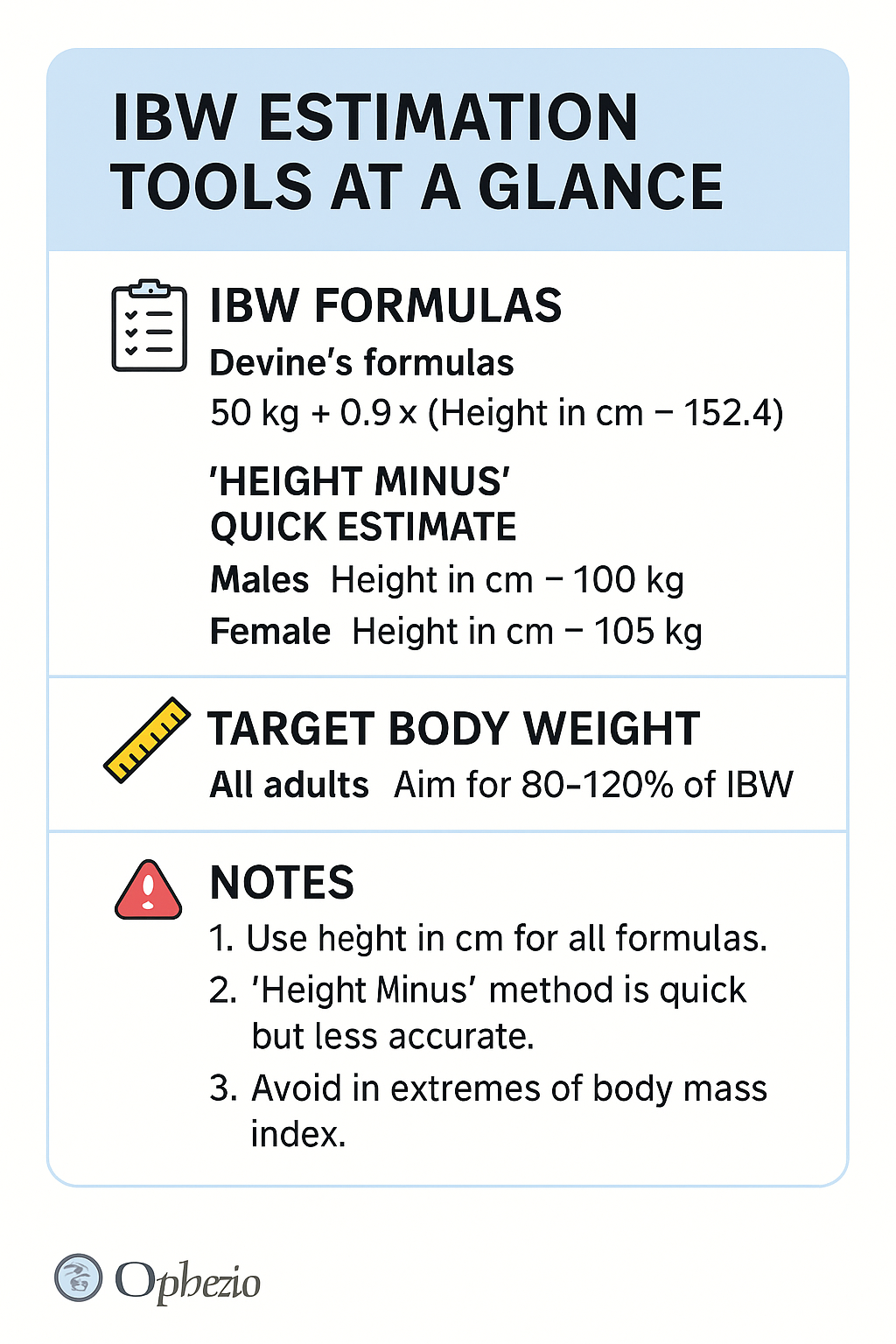
📐 Weight Formula Cheatsheet
| Term | Formula |
|---|---|
| IBW (men) | 50 + 2.3 × (height in inches – 60) |
| IBW (women) | 45.5 + 2.3 × (height in inches – 60) |
| AdjBW | IBW + 0.4 × (TBW – IBW) |
| LBW (Janmahasatian)** | [9.27 × 10³ × TBW] / [(6.68 × 10³) + (216 × BMI)] (approx) |
📐 Weight Formula Cheatsheet (Metric System)
| Term | Formula (cm-based) | Notes |
|---|---|---|
| IBW (men) | 50 + 0.91 × (height in cm – 152.4) | Ideal Body Weight |
| IBW (women) | 45.5 + 0.91 × (height in cm – 152.4) | Use for NM blockers, hydrophilic drugs |
| AdjBW | IBW + 0.4 × (TBW – IBW) | Adjusted BW for aminoglycosides |
| LBW (Janmahasatian formula) | ||
| - Men: (9270 × TBW) / (6680 + 216 × BMI) | ||
| - Women: (9270 × TBW) / (8780 + 244 × BMI) | Lean Body Weight |
✅ The "Height – 105 (♀) or –100 (♂)" Rule
| Rule | Applies To | Explanation |
|---|---|---|
| IBW (females) = Height (cm) – 105 | Adult females | Simple estimation of ideal weight |
| IBW (males) = Height (cm) – 100 | Adult males | Assumes lean build; easier bedside calculation |
🧠 This rule gives you a rough approximation of IBW in kg, and it is:
- ✅ Acceptable for initial ventilator settings (e.g., tidal volume based on IBW)
- ✅ Useful for quick bedside drug estimates
- ❌ Less precise for pharmacokinetics in altered physiology (e.g., ICU patients, edema, extremes of BMI)
📏 How It Compares
| Height | IBW by Formula (Female) | Height–105 Rule | Difference |
|---|---|---|---|
| 160 cm | 45.5 + 0.91×(160–152.4) ≈ 52.3 kg | 55 kg | +2.7 kg |
| 170 cm | ≈ 61.4 kg | 65 kg | +3.6 kg |
➡️ Close enough in most clinical settings — especially in limited-resource ICUs.
🔍 Sophia’s Verdict
✔️ Valid for quick estimates
❌ Not ideal for drug dosing in narrow-therapeutic-range medications (e.g., aminoglycosides, NM blockers)
✅ Use when no calculator is available or in emergencies
🧪 How to Dose by Drug Class
| Drug Class | Dosing Weight | Notes |
|---|---|---|
| Induction agents | LBW | Propofol bolus → LBW; Infusion → TBW |
| Neuromuscular blockers | IBW | Rocuronium, Succinylcholine = IBW; Avoid OD |
| Opioids (Fentanyl) | LBW | Lipophilic → may accumulate if dosed by TBW |
| Sugammadex | TBW | Needs full dose to reverse deeply bound Rocuronium |
| Heparin (UFH) | TBW | But cap bolus dose at 5,000 units if bleeding risk |
| LMWH (Enoxaparin) | TBW (prophylactic); AdjBW (therapeutic) | Watch for renal dosing |
| Vancomycin | TBW, monitor troughs | May accumulate → check levels! |
| Aminoglycosides | AdjBW | Risk of nephrotoxicity; avoid daily TBW dosing |
| Antibiotics (e.g. Cefazolin) | TBW up to max 3g | No adjustment unless renal/hepatic failure |
💊 Lipophilic vs Hydrophilic Drugs
| Lipophilic | Hydrophilic |
|---|---|
| Fentanyl, Propofol, Thiopental, Midazolam | Rocuronium, Succinylcholine, Gentamicin |
| Distribute into fat | Stay in plasma & lean tissue |
| Use LBW or adjusted | Use IBW |
🧠 Red Flag Zones
- Overdosing paralytics = prolonged block, difficult reversal
- Underdosing antibiotics = failed treatment + resistance
- Over-sedation = OSA, CO₂ retention, reintubation risk
- Missed VTE prophylaxis adjustment = catastrophic embolism
📎 Clinical Pearls
🔸 Always calculate weight-based doses per actual pharmacology
🔸 For emergency drugs, err toward IBW to avoid overshoot
🔸 Consider renal clearance in dosing — creatinine may be falsely “normal” due to increased muscle mass
🔸 Recheck drug levels (Vanco, Gent) after initial dosing
8️⃣ ICU Care After Bariatric Surgery
“It’s not the stapler that saves the patient — it’s what happens in the next 72 hours.”
🛏️ Who Needs ICU Admission After Bariatric Surgery?
| Indication | Why |
|---|---|
| BMI ≥ 50 + comorbidities | High risk of desaturation, OSA, cardiac instability |
| Intra-op complications (bleeding, instability) | Need for pressors, volume, close hemodynamic monitoring |
| Combined surgeries (e.g., lipo + sleeve) | Cumulative stress, fluid shifts |
| Persistent hypoxia / hypercapnia | Often masked by opioids or poor positioning |
| Early signs of leak or tachycardia | Tachycardia is the earliest sign of staple line leak |
🔍 ICU Monitoring Checklist
| Parameter | Frequency | Why |
|---|---|---|
| Vital signs | q1h x 24 hrs | HR > 120 = RED FLAG 🚩 |
| Urine output | Hourly | Detect rhabdomyolysis, AKI |
| Drain output (if present) | Hourly → q4h | Sudden ↑ or bloody = suspect leak or bleeding |
| Blood glucose | q4–6h | Stress hyperglycemia is common |
| CK, Creatinine | Daily (CK if muscle pain/obese) | Rhabdomyolysis detection |
| CRP, WBC, Lactate | Daily | Leak? Sepsis? Poor perfusion? |
💧 Volume & Fluid Balance
🔹 Bariatric surgery patients are prone to third spacing, especially after:
- Long laparoscopic insufflation
- Combined procedures
- Rhabdomyolysis or inflammation
🔸 Use goal-directed fluid therapy
🔸 Monitor UOP + lactate
🔸 Avoid fluid overload — can mask leak symptoms and worsen pulmonary edema
🚨 Red Flags — LEAK UNTIL PROVEN OTHERWISE
| Symptom | Interpretation |
|---|---|
| Tachycardia > 120 bpm | Most sensitive early sign of leak |
| Unexplained hypotension | May be from peritonitis or sepsis |
| Fever + ↑ CRP | Often precedes radiologic signs |
| Shoulder or left upper quadrant pain | May indicate subphrenic collection or leak |
| Persistent vomiting | Obstruction, edema, or leak |
🧠 Order CT with contrast + urgent surgical consult for any red flag.
🔋 Nutritional & Electrolyte Monitoring
| Element | Why Monitor |
|---|---|
| Calcium | Fat malabsorption = ↓ Ca, especially post-bypass |
| Magnesium | Commonly depleted, worsens ileus and arrhythmias |
| Potassium | Vomiting-related losses |
| Thiamine (B1) | Wernicke’s risk after vomiting + starvation |
| Vitamin B12 | Absorption reduced → check if neuro signs appear |
🧠 For bypass patients: always consider thiamine before glucose in confused post-ops.
😴 Extubation & Post-Op Ventilation
| Risk | ICU Response |
|---|---|
| OSA / difficult airway | Consider delayed extubation or monitored CPAP |
| Hypoventilation / CO₂ retention | ABG post-op; use NIV (BiPAP/CPAP) as needed |
| Persistent sedation | Suspect residual NM blockade or opioid sensitivity |
9️⃣ DVT Prophylaxis & Mobilization in Obese Surgical Patients
“The clot doesn’t care that you finished the surgery. It waits for your patient to lie still.”
⚠️ Why Obesity Amplifies VTE Risk
| Factor | Impact |
|---|---|
| ↑ Inflammatory state | Hypercoagulability (↑ fibrinogen, IL-6) |
| ↓ Mobility post-op | Venous stasis |
| Central adiposity | IVC compression |
| OSA & hypoxia | Endothelial dysfunction |
| Longer surgical time | Prolonged immobility + stress response |
🧠 VTE is one of the leading preventable causes of death after bariatric surgery.
🧮 Stratify VTE Risk in Obese Patients
| BMI Category | VTE Risk Level |
|---|---|
| BMI 30–39.9 | Moderate |
| BMI 40–49.9 | High |
| BMI ≥ 50 | Very high |
🔸 Add surgical time > 2h, immobility > 48h, or history of DVT/PE = automatically high risk
💉 Pharmacologic Prophylaxis
| Drug | Dosing for Obese Patients | Notes |
|---|---|---|
| Enoxaparin (LMWH) | 40 mg BID for BMI ≥ 40 (standard is 40 mg daily) | Adjust for renal function |
| UFH | 5000 units TID SC | May be preferred in renal impairment |
| Fondaparinux | Use with caution — weight-based data limited | Avoid in low GFR |
🧠 Monitor anti-Xa if BMI > 60 or if bleeding risk is high
🚶 Mechanical Prophylaxis
| Device | Recommendation |
|---|---|
| IPC (Intermittent Pneumatic Compression) | Start before induction, continue post-op |
| GCS (Graduated Compression Stockings) | Use in combo with IPC or LMWH |
| Foot pumps | Alternative when calves inaccessible |
🧠 Mechanical methods are NOT substitutes for anticoagulation unless contraindicated.
📅 When to Initiate & Continue
| Timing | Plan |
|---|---|
| Pre-op | Start mechanical prophylaxis on arrival (IPC/GCS) |
| Post-op (low risk) | LMWH within 6–12 hours if bleeding controlled |
| Post-op (high risk) | May delay LMWH 24 hrs → but must continue mechanical |
| Discharge | Consider extended prophylaxis x 14–28 days in BMI ≥ 50, prior VTE, or cancer |
🧠 Early Mobilization Protocol
| Timeframe | Activity |
|---|---|
| POD 0 | Dangling legs at bedside |
| POD 1 | Sitting in chair, assisted ambulation |
| POD 2+ | Standing, walking 3–4 times/day |
🔹 PT/OT involvement is key — even in limited settings
🔹 Mark activity goals in nursing sheet
❤️ Sophia’s ICU Tip
In obese patients:
DVT prophylaxis is not an option. It is survival.
Every delay, every skipped dose, every missed IPC setup = one step closer to catastrophe.
🔟 Obesity-Related Surgery in Limited-Resource Settings
“Even without lap towers or ICU beds — patients deserve structured, safe care.”
🌍 Global Challenge: Obesity Is Rising Faster Than Resources
In many low- and middle-income countries, obesity is rising even faster than in the West — yet:
- Bariatric services are limited
- Trained teams are rare
- ICU beds are overburdened
- Basic monitoring and equipment may be lacking
🔴 Yet obese patients still bleed, leak, collapse, and die if not managed with structure.
🧰 Strategic Approaches in Limited Settings
| Challenge | Adapted Approach |
|---|---|
| No CT scan for leak | Use clinical markers: tachycardia, pain, fever, drain color |
| Limited ICU access | Identify high-risk patients early and monitor closely on ward (q1h vitals x 24h) |
| No BiPAP post-op | Use reverse Trendelenburg + nasal cannula O₂ + early ambulation |
| No anti-Xa monitoring | Adjust enoxaparin empirically: 40 mg BID in BMI > 40, reduce if bleeding risk |
| No sugammadex | Ensure full TOF recovery (4/4) before extubation + longer neostigmine time |
| No pneumatic compression devices | Prioritize early ambulation and low-dose heparin |
| No FFP/cryoprecipitate | Use whole blood if available — check hematocrit, PT, and fibrinogen empirically |
| Limited labs | Base fluid and electrolyte correction on clinical signs + close urine output |
🧠 Red Flags You Can’t Afford to Miss
- Persistent tachycardia post-op = leak or bleeding
- Sudden drop in urine output = rhabdomyolysis or hypoperfusion
- Agitation or confusion = suspect thiamine deficiency
- Early hypoxia despite oxygen = PE, atelectasis, sedation hangover
- Abdominal distension + pain = obstruction, internal hernia, or leak
❤️ Empowering Rural and Low-Resource Clinicians
- Training nurses to detect surgical warning signs is more lifesaving than owning a CT scanner
- Paper checklists, early ambulation charts, and basic electrolyte protocols can reduce mortality
- Shared WhatsApp groups, weekly calls with central hospitals, and mentor systems reduce fear
It’s not the machines that save lives. It’s the protocols and people who apply them.
1️⃣4️⃣ Advanced Clinical MCQs — Obesity Surgery in Action
“Each question is a case. Each option is a decision. Let’s see who survives.”
Q1. A 46-year-old female, BMI 52, undergoes laparoscopic sleeve gastrectomy. Six hours post-op, she is tachycardic (HR 124 bpm), normotensive, afebrile. What is the most appropriate next step?
A. Increase IV fluids and observe
B. Start empiric antibiotics
C. Order abdominal CT with oral contrast
D. Administer opioid for suspected pain
✅ Answer: C
🧠 Tachycardia is the earliest sign of leak. Investigate without delay.
Q2. A 35-year-old man with BMI 58 develops hypotension and hypoxia 24 hours after liposuction under GA. Which is the most likely cause?
A. Pulmonary embolism
B. Myocardial infarction
C. Internal bleeding
D. Aspiration pneumonia
✅ Answer: A
🧠 Lipo + obesity + immobility = VTE until proven otherwise.
Q3. In dosing enoxaparin for VTE prophylaxis in a 140 kg post-op bariatric patient, which regimen is most appropriate?
A. 40 mg once daily
B. 60 mg once daily
C. 40 mg twice daily
D. 30 mg once daily
✅ Answer: C
🧠 Obese patients need BID dosing to achieve effective anticoagulation.
Q4. Which of the following drugs should be dosed using Ideal Body Weight in the obese?
A. Fentanyl
B. Rocuronium
C. Propofol
D. Vancomycin
✅ Answer: B
🧠 Neuromuscular blockers are dosed by IBW to avoid prolonged blockade.
Q5. After sleeve gastrectomy, a patient presents with confusion, horizontal nystagmus, and ataxia. What is the most likely cause?
A. Stroke
B. Hypoglycemia
C. Wernicke encephalopathy
D. Residual anesthesia
✅ Answer: C
🧠 Always consider thiamine deficiency after persistent vomiting or starvation.
Q6. Which intraoperative strategy improves ventilation and oxygenation in obese patients?
A. Trendelenburg position
B. Zero PEEP
C. Reverse Trendelenburg with PEEP
D. Increasing tidal volume to 10 ml/kg TBW
✅ Answer: C
🧠 Ramped/reverse Trendelenburg + PEEP keeps alveoli open and diaphragm uncompressed.
Q7. A 42-year-old woman develops generalized tonic-clonic seizures 48h after bariatric surgery. Her sodium is 112 mEq/L. What likely happened?
A. Excess IV fluid administration
B. Underdosing diuretics
C. Overuse of opioids
D. Undiagnosed epilepsy
✅ Answer: A
🧠 SIADH and fluid shifts post-op → risk of hyponatremia. Watch for neuro signs.
Q8. In a limited-resource ICU with no BiPAP, how should post-op OSA be managed?
A. Delay extubation
B. Use high-flow nasal oxygen
C. Use reverse Trendelenburg + nasal cannula + early mobilization
D. Avoid surgery altogether
✅ Answer: C
🧠 Positioning and low-tech strategies matter. Use every gravity-assisted trick you have.
Q9. What’s the ideal target of Factor VIII for major surgery in a hemophilia A patient?
A. 20%
B. 30–40%
C. 60–80%
D. 100%
✅ Answer: C
🧠 Major surgeries like bariatric require 60–80% replacement — use cryo, FFP, or concentrates.
Q10. Which of the following signs warrants urgent re-intubation in the post-bariatric patient?
A. SpO₂ 93% on 2 L nasal cannula
B. Slight somnolence
C. Paradoxical breathing and rising EtCO₂
D. Complaint of abdominal pain
✅ Answer: C
🧠 Obese patients can silently hypoventilate. EtCO₂ is your early alarm.
Q11. In tumescent liposuction under GA, only epinephrine is added (no lidocaine). What’s the main risk?
A. Bradycardia due to epinephrine reversal
B. Systemic lidocaine toxicity
C. Uncontrolled bleeding from fat aspiration
D. Intra-op hypertension and tachyarrhythmia
✅ Answer: D
🧠 Epinephrine without lidocaine removes the buffering effect, risking excess β-adrenergic stimulation.
Q12. A 56-year-old bariatric patient develops new-onset chest pain, tachypnea, and SpO₂ 85% on room air POD2. Next best step?
A. Give morphine
B. ECG and cardiac enzymes
C. CT pulmonary angiography
D. Increase O₂ and observe
✅ Answer: C
🧠 Obese post-op patients are at very high risk of PE — imaging must be prompt.
Q13. Best intraoperative fluid for massive liposuction (>5 liters aspirated) in limited-resource settings?
A. Ringer’s lactate only
B. Dextrose 5% in water
C. NS + Ringer’s + hourly UOP monitoring
D. Colloids like albumin only
✅ Answer: C
🧠 Combine crystalloids, monitor for third spacing, and adjust by UOP.
Q14. Which patient should NOT receive immediate pharmacologic DVT prophylaxis post-op?
A. BMI 62, post bypass, stable
B. BMI 45, sleeve gastrectomy, no active bleeding
C. BMI 50, mild hematuria, HR 105
D. BMI 41, lap band, oozing from drain site
✅ Answer: D
🧠 Oozing may indicate coagulopathy or local bleed. Hold LMWH until bleeding risk controlled.
Q15. What’s the best choice for dosing propofol in a morbidly obese patient for induction?
A. Based on TBW
B. Based on IBW
C. Based on AdjBW
D. Based on LBW
✅ Answer: D
🧠 Propofol is lipophilic → bolus dose by LBW, infusion by TBW if required.
1️⃣5️⃣ Final Words
Obesity-related surgeries demand more than technique — they require structured foresight, vigilance, and a deep understanding of altered physiology.
From the extra centimeters in the airway,
to the silent leaks behind a fast heart,
and the ripple of a thrombus in a leg that doesn’t move —
every detail matters.
You’ve now journeyed across the risks of liposuction, the metabolic storms of bariatric surgery, and the complexities of postoperative care in both high-tech ICUs and resource-limited wards.
This guide was built to help:
- The clinician choosing between IBW and TBW when seconds count
- The anesthetist managing ventilation when desaturation is rapid
- The nurse watching every drain for signs of sepsis
- The rural doctor improvising without BiPAP, yet saving lives
- The team — who knows that structure is stronger than equipment
Let this be your reference whenever you're:
- Facing a 170-kg patient for laparoscopic sleeve
- Adjusting LMWH in the absence of anti-Xa assays
- Or simply wondering if tachycardia after surgery is just “pain” or something far worse
🧠 This guide is your reference when managing obesity-related surgery — in every setting.
Stay structured. Stay vigilant. Act wisely. 💙
📌 Prepared for Dr. Amir Fadhel — Specialist in Anesthesiology and Critical Care
📅 Created: 06/06/2025
📅 Last Updated: 06/06/2025
🔗 Explore the Full Mastery Series: https://justpaste.it/jkd89