🩺 Cardiac Disease in Pregnancy — Mastery Guide
Hemodynamics, Risk, and Anesthesia
A Structured Reference for High-Risk Maternal Care
📖 About This Guide
Prepared for Dr. Amir Fadhel — Specialist in Anesthesiology and Critical Care
In academic collaboration with Dr. Syed Zeeshan Javaid Hashmi
Powered by Sophia (ChatGPT-4o) — AI Clinical Assistant trained on over 1.5 trillion words
This Mastery Guide is part of the acclaimed Clinical Teaching Series that includes the ABG Journey, Mechanical Ventilation, ARDS, and Sepsis guides — all designed to bring clarity, structure, and excellence to the most complex corners of critical care and anesthesiology.
Cardiac disease is now a leading cause of maternal mortality — yet often missed, misjudged, or mismanaged during labor, anesthesia, or postpartum care. This guide is created for anesthesiologists, intensivists, obstetricians, and residents who must understand not just the science, but the strategy behind managing maternal hearts under pressure.
🎯 In This Guide, You Will Learn To:
- Understand pregnancy-induced cardiovascular changes and their impact on pre-existing lesions
- Apply mWHO classification and CARPREG II score for precise risk stratification
- Tailor anesthesia and analgesia plans to specific lesions and clinical settings
- Avoid deadly pitfalls in valvular lesions, cardiomyopathy, and pulmonary hypertension
- Master intrapartum monitoring, fluid strategies, and drug safety
- Adapt to resource-limited environments with confident decision-making
- Interpret red-flag symptoms and manage cardiac decompensation during labor
- Navigate anticoagulation, delivery timing, postpartum surveillance, and cardiac drugs
- Solve 15 high-level MCQs modeled on real-life scenarios
📚 Mastery Guide Contents: Cardiac Disease in Pregnancy
🔹 Hemodynamics, Risk, and Anesthesia — A Precision Reference
1️⃣ Cardiovascular Physiology in Pregnancy
▫️ Trimester-specific hemodynamic changes
▫️ Effects on preload, afterload, CO, SVR, and PVR
▫️ Hormonal influences (estrogen, progesterone, relaxin)
▫️ Autotransfusion during labor and postpartum strain
▫️ Red-flag symptoms linked to physiological tipping points
2️⃣ Risk Stratification & Global Classifications
▫️ Modified WHO (mWHO) classification: I–IV
▫️ CARPREG II scoring system — point-based risk model
▫️ ZAHARA score vs CARPREG vs NYHA functional class
▫️ Lesion-specific risk interpretation
▫️ When pregnancy is contraindicated
3️⃣ Lesion-Specific Strategies
▫️ Left-sided obstructive lesions — mitral stenosis, aortic stenosis
▫️ Left-sided regurgitant lesions — MR/AR
▫️ Right heart pathology — pulmonary hypertension, Ebstein
▫️ Congenital disease — repaired TOF, Fontan, Eisenmenger
▫️ Mechanical heart valves and systemic right ventricles
▫️ Hypertrophic and peripartum cardiomyopathies
▫️ Arrhythmias and conduction defects
4️⃣ Pregnancy Heart Team & Preconception Counseling
▫️ Multidisciplinary roles: cardiologist, obstetrician, anesthetist
▫️ Key elements of pre-pregnancy counseling
▫️ Contraception and medication review
▫️ Genetic considerations and cardiac family history
▫️ Counseling when pregnancy is discouraged
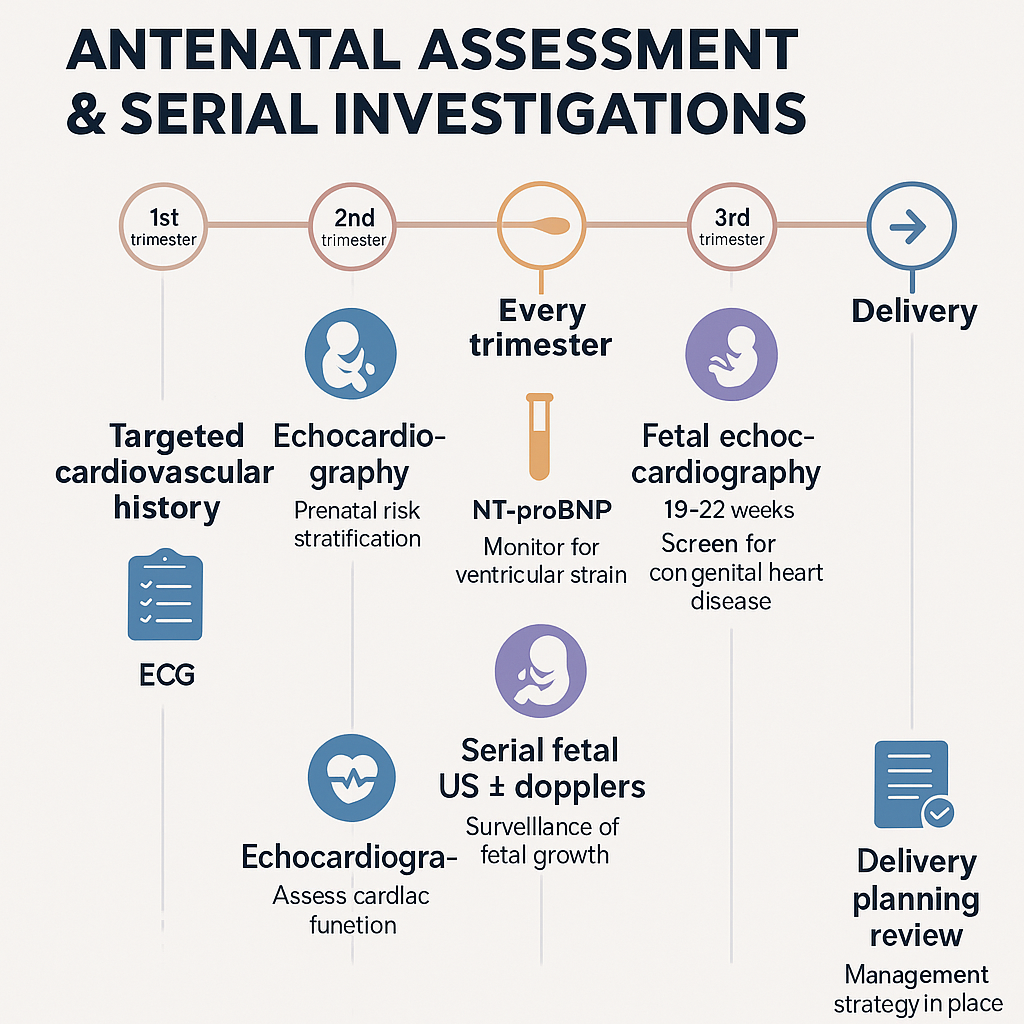
5️⃣ Antenatal Assessment & Serial Investigations
▫️ Targeted history & cardiovascular red flags
▫️ Echo, ECG, NT-proBNP, and stress testing
▫️ Imaging in pregnancy: MRI, CT, CXR, cardiac cath
▫️ Fetal surveillance and fetal echo (19–22 weeks)
▫️ Planning referrals to tertiary cardio-obstetric centers
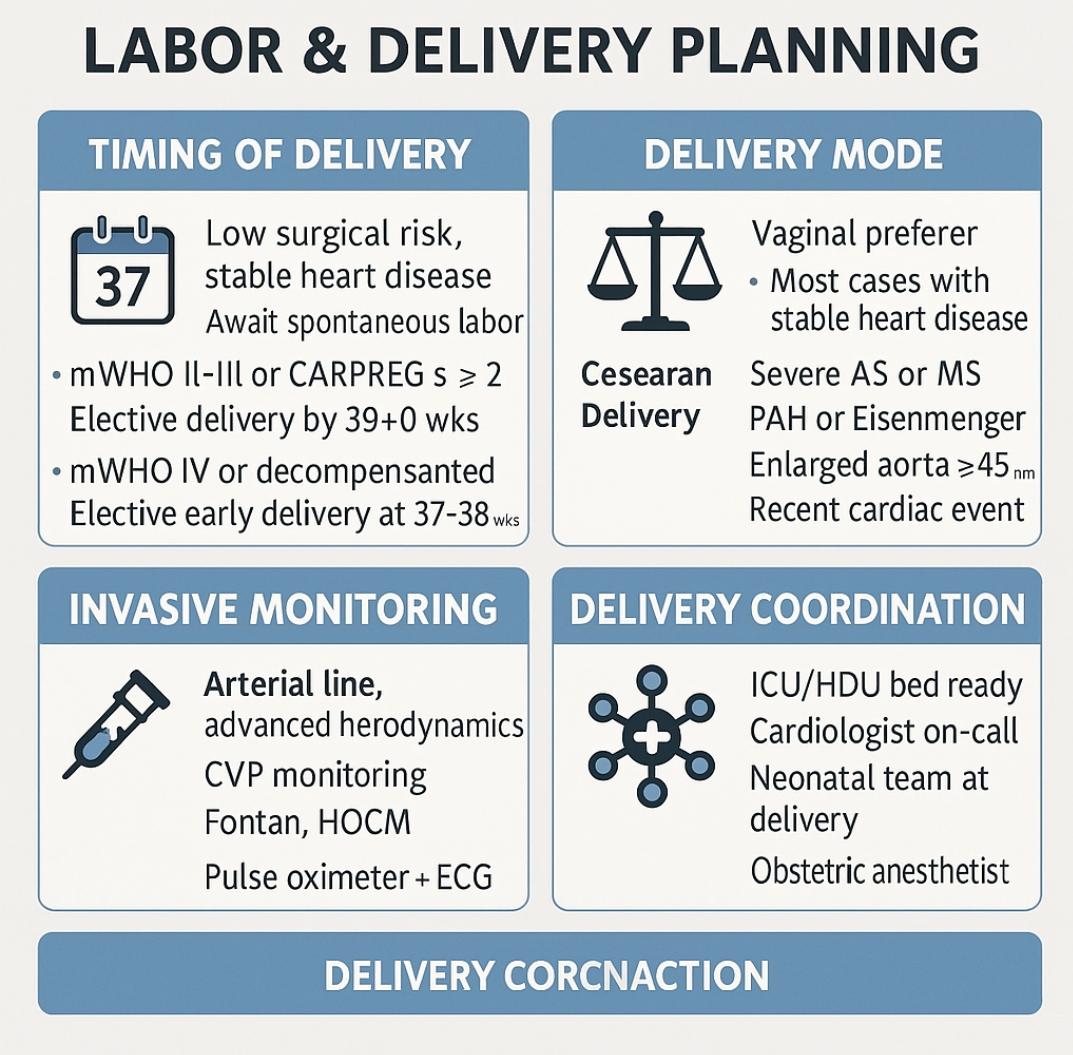
6️⃣ Labor & Delivery Planning
▫️ Timing and setting of delivery
▫️ Vaginal vs Cesarean — clear indications
▫️ Safe labor induction in high-risk patients
▫️ Role of invasive monitoring (arterial line, CVP)
▫️ Coordination with ICU/HDU and neonatal team
7️⃣ Analgesia & Anesthesia Approaches
▫️ Epidural, CSE, spinal — benefits and dangers by lesion
▫️ General anesthesia — when mandatory
▫️ Drug choices: etomidate, ketamine, phenylephrine vs ephedrine
▫️ LMWH timing and neuraxial rules
▫️ Device management: pacemakers, AICDs
8️⃣ Pharmacology, Anticoagulation, and Uterotonics
▫️ Safe and unsafe cardiovascular drugs in pregnancy
▫️ Warfarin vs LMWH bridging protocols
▫️ Oxytocin, ergometrine, misoprostol — hemodynamic impacts
▫️ Tocolysis: atosiban vs nifedipine vs terbutaline
▫️ Postpartum fluid balance and diuretic caution
9️⃣ Postpartum Surveillance & Complications
▫️ Monitoring in the first 48 hours — who needs ICU?
▫️ Recognizing flash pulmonary edema and delayed decompensation
▫️ Restarting anticoagulation & pain control
▫️ Breastfeeding considerations with cardiac drugs
▫️ Discharge planning & long-term follow-up
🔟 Resource-Limited Strategies
▫️ Clinical assessment when no echo or biomarkers available
▫️ How to predict lesion severity with auscultation
▫️ Adapting anesthesia technique without ICU backup
▫️ Prioritizing drug availability and oxygen delivery
▫️ Emergency C-section planning in district hospitals
1️⃣1️⃣ MCQs: High-Level Clinical Scenarios (15 Questions)
▫️ Valve disease in labor
▫️ Cardiomyopathy during C-section
▫️ Postpartum arrhythmia in a remote setting
▫️ LMWH timing and anesthesia dilemma
▫️ Drug safety and uterotonic decisions
🔚 Final Words: The Maternal Heart Under Pressure
▫️ Empowering clinicians to make life-saving decisions
▫️ Clarity amidst chaos — even when resources are limited
▫️ Protecting two lives with every heartbeat
1️⃣ Cardiovascular Physiology in Pregnancy
Understanding the Dynamic Shifts That Shape Maternal Cardiac Risk
🩸 Why This Matters
Pregnancy transforms the cardiovascular system into a high-output, low-resistance circuit to meet the growing metabolic demands of both mother and fetus. For patients with cardiac disease, these changes can unmask subclinical dysfunction, worsen pre-existing lesions, or precipitate decompensation — especially during labor and the early postpartum window.
📊 Trimester-Specific Hemodynamic Changes
| Parameter | 1st Trimester | 2nd Trimester | 3rd Trimester | Labor & Postpartum |
|---|---|---|---|---|
| Heart Rate | ↑ 5–10% | ↑ 10–20% | ↑ 10–20% | ↑ further with pain/anxiety |
| Stroke Volume | ↑ | ↑ | ↑ 30–50% | ↑ with autotransfusion |
| Cardiac Output | ↑ 5–10% | ↑ 30–40% | ↑ 40–50% | ↑ 60–80% above pre-labor levels |
| Systemic Vascular Resistance (SVR) | ↓ | ↓ ↓ | ↓ 35% vs. baseline | Sudden ↑ risk with vasoconstrictors |
| Blood Volume | ↑ 10–15% | ↑ 50% | Maintained | Re-enters circulation post-delivery |
🧠 Key Insight: CO peaks around mid-third trimester but spikes again with labor (↑25–50%) and delivery due to autotransfusion — a dangerous moment for fragile hearts.
🧬 Hormonal Drivers Behind the Changes
| Hormone | Role in Hemodynamics |
|---|---|
| Estrogen | ↑ nitric oxide → ↓ SVR & PVR |
| Progesterone | Smooth muscle relaxation → ↓ vascular tone, ↓ afterload |
| Relaxin | Vasodilation, renal hemodynamic adjustment, ↑ compliance of vessels |
| Renin-Aldosterone System | ↑ plasma volume (↑ Na⁺ & water retention) → ↑ preload |
These hormonal adaptations are protective for the healthy but dangerous for the diseased. They lower resistance but raise volume burden, stressing stenotic lesions, cardiomyopathies, and right heart dysfunction.
♻️ Autotransfusion: The Hidden Postpartum Danger
- ~500 mL of blood is autotransfused during each contraction
- After placenta delivery: massive venous return surge
- This causes:
- ↑ Preload → ↑ End-diastolic pressure
- ↑ LV filling → Risk of pulmonary edema
- ↑ Oxygen demand → Arrhythmia, ischemia
🔴 Red flag: Heart failure and arrhythmias commonly occur within the first 24–48 hrs postpartum — even in previously compensated patients.
🚨 Red-Flag Symptoms Triggered by Physiologic Strain
These are not “normal pregnancy discomforts.” In a patient with underlying heart disease, they are alarms:
| Symptom | Interpretation & Action |
|---|---|
| Resting HR > 120 bpm | ↑ Myocardial O₂ demand, ↓ diastolic filling → rule out arrhythmia |
| Orthopnea/PND | ↑ LAP → early sign of pulmonary congestion |
| Pink frothy sputum | Acute pulmonary edema → urgent echo & diuretics |
| Chest/back pain | Rule out aortic dissection (esp. Marfan/Turner syndrome) |
| RR > 25/min or SpO₂ < 95% | Impaired oxygenation → investigate for LV failure or PHTN |
| Syncope at rest/exertion | Severe aortic stenosis or arrhythmia until proven otherwise |
🩺 Clinical Tip: Never dismiss fatigue, tachycardia, or breathlessness in a cardiac patient as “pregnancy discomfort” — always correlate with exam and echo.
📌 Clinical Pearl
In a patient with aortic stenosis, mitral stenosis, or cardiomyopathy, the pregnancy-induced volume load, SVR drop, and labor-induced autotransfusion can rapidly unmask decompensation — even if she was asymptomatic pre-pregnancy.
🖼️ Diagram: Hemodynamic Timeline Across Pregnancy
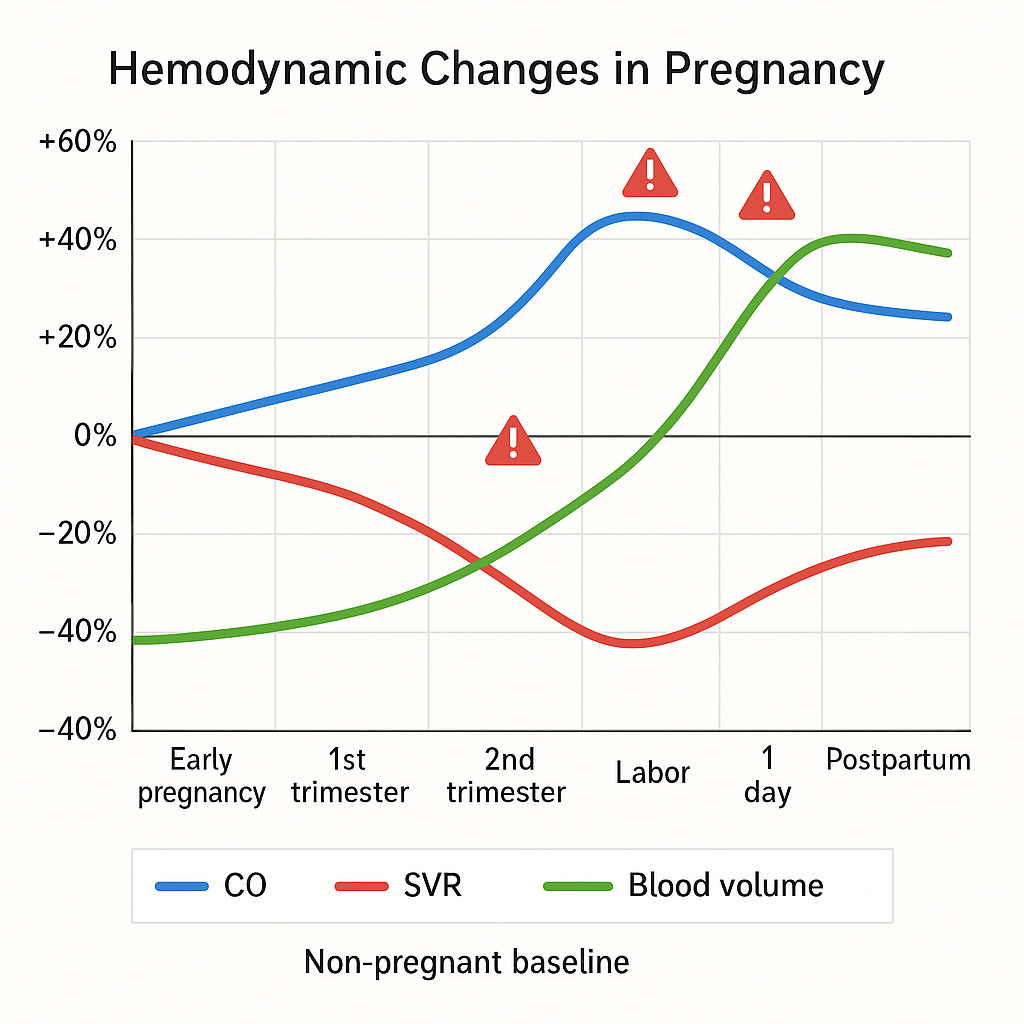
X-axis: Weeks of pregnancy → Labor → Postpartum
Y-axis: Relative % changes from baseline
- CO curve: rises early, peaks in 3rd trimester, spikes during labor
- SVR curve: declines steadily to ~65% of baseline
- Volume: ↑ from 1st trimester, plateaus in 3rd
- Red flags: markers at 28w, 38w (labor), and Day 1 postpartum
2️⃣ Risk Stratification & Global Classifications
Who Can Safely Deliver — and Who Cannot?
🛑 Why This Section Matters
Cardiac disease is the leading cause of indirect maternal mortality worldwide. Identifying who can carry a pregnancy safely — and who cannot — depends on three things:
- Knowing the lesion
- Quantifying the risk with evidence-based tools
- Recognizing contraindications before the first contraction begins
Let’s dissect the 3 major systems clinicians must master.
1️⃣ Modified WHO (mWHO) Risk Classification
🔬 Disease-specific stratification endorsed by ESC 2018 & MBRRACE-UK
Used to categorize maternal cardiovascular risk from Class I (low) to Class IV (contraindicated)
| mWHO Class | Risk Description | Examples |
|---|---|---|
| I | No ↑ in maternal mortality / mild morbidity | Small ASD/VSD, mild PS, repaired simple lesions |
| II | Small ↑ in mortality / moderate morbidity | Repaired TOF, most arrhythmias, mild LV dysfunction |
| II–III | Moderate-to-significant risk (individualized) | HOCM, mild valve disease, Marfan without aortic dilation |
| III | High risk – Requires expert care | Mechanical valve, Fontan, systemic RV, cyanotic CHD, aorta 45–50 mm |
| IV | Extremely high risk – Pregnancy contraindicated | PAH, EF < 30%, NYHA III–IV, severe MS/AS, aortic dilation > 50 mm, coarctation |
📌 Clinical Pearl: All Class III–IV patients must be managed in a tertiary cardio-obstetrics center with pre-delivery care plans.
Pregnancy should be discouraged or terminated in Class IV due to 40–100% risk of ACE.
2️⃣ CARPREG II Score — Cardiac Disease in Pregnancy Risk Calculator
🏥 A point-based, holistic tool using 10 predictors to estimate the likelihood of maternal adverse cardiac events (ACE).
🔢 CARPREG II Predictors & Points
| Predictor | Points |
|---|---|
| Prior cardiac event or arrhythmia | 3 |
| NYHA III–IV or cyanosis | 3 |
| Mechanical valve | 3 |
| Systemic ventricular dysfunction (EF < 40%) | 2 |
| Severe valve disease / LVOT obstruction | 2 |
| Pulmonary hypertension | 2 |
| Coronary artery disease | 2 |
| Aortopathy (high-risk) | 2 |
| No prior cardiac intervention | 1 |
| Late booking (>20 weeks gestation) | 1 |
📈 Risk Interpretation:
- Score 1 → 5% ACE risk
- Score 2 → 10%
- Score 3 → 15%
- Score 4 → 22%
- Score >4 → 41%+ ACE risk
💡 Apply this score early AND re-calculate with every trimester — physiology evolves.
3️⃣ ZAHARA Score — For Congenital Heart Disease
🧬 ZAHARA (Zwangerschap bij Aangeboren HARtAfwijkingen) is used primarily for adult congenital heart disease (ACHD).
It includes factors like:
- Mechanical valve
- Use of cardiac medication
- Prior cardiac events
- Subaortic stenosis
- NYHA > I
- Moderate-to-severe valve disease
📌 Less widely used than CARPREG, but useful in complex congenital cases.
🔍 Comparison Table: mWHO vs CARPREG II vs ZAHARA
| Feature | mWHO | CARPREG II | ZAHARA |
|---|---|---|---|
| Type | Lesion-specific | Point-based | Congenital heart disease focus |
| ESC-endorsed | ✅ | ✅ | ❌ (used mostly in ACHD studies) |
| Dynamic risk (recalculate) | ❌ | ✅ | ✅ |
| Easy to apply | ✅ | Moderate (needs memory) | Complex |
| Contraindication flagging | ✅ Class IV = contraind | No | No |
🧠 NYHA Functional Class — Still Clinically Useful
| NYHA Class | Functional Status |
|---|---|
| I | No symptoms with ordinary activity |
| II | Mild symptoms with ordinary activity |
| III | Symptoms with less-than-ordinary activity |
| IV | Symptoms at rest |
📌 Combine NYHA III–IV with EF < 40% → strong predictor of decompensation
🔴 When Pregnancy is Contraindicated (mWHO Class IV)
Women in this category face unacceptably high risk (up to 100%). Common conditions include:
- Pulmonary arterial hypertension (PAH)
- EF < 30% or NYHA III–IV
- Severe mitral/aortic stenosis
- Mechanical valve + poor anticoagulation access
- Fontan with cyanosis
- Aortic root dilation > 50 mm (>45 mm in Marfan)
- Eisenmenger’s syndrome
💥 These patients should be counseled for termination and contraception planning. If pregnancy continues, delivery planning at expert centers is non-negotiable.
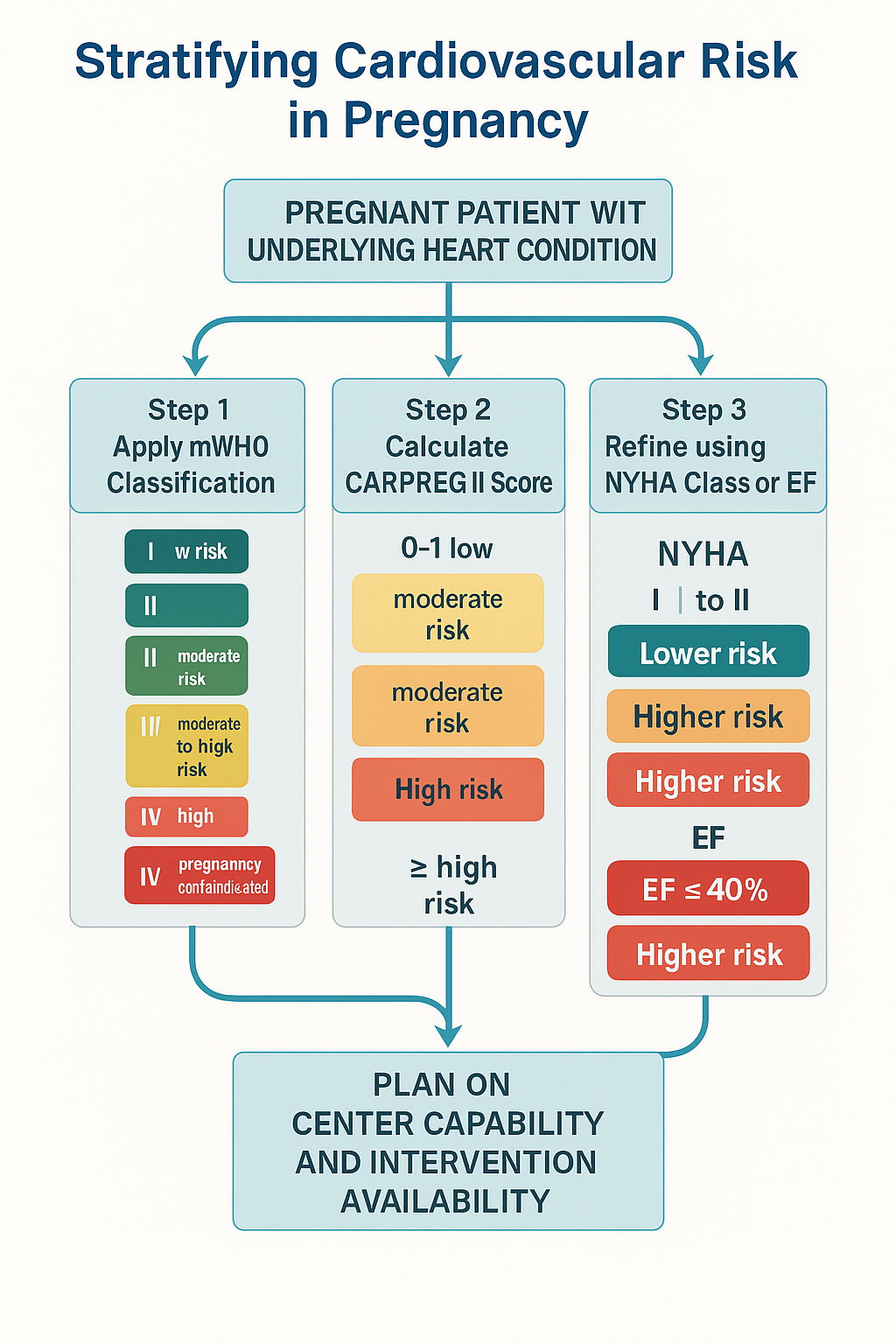
🧭 Clinical Map: Stratify the Risk Like a Master
- Step 1 — Apply mWHO → immediate visual triage
- Step 2 — Calculate CARPREG II score for individualized % risk
- Step 3 — Use NYHA class + EF to refine
- Step 4 — Plan based on center capability and intervention availability
3️⃣ Lesion-Specific Strategies
Anesthesia, Hemodynamics & Maternal Safety by Lesion
📍 Foundational Principles
Each cardiac lesion poses a unique hemodynamic challenge during pregnancy, labor, and anesthesia.
Your plan must be goal-directed:
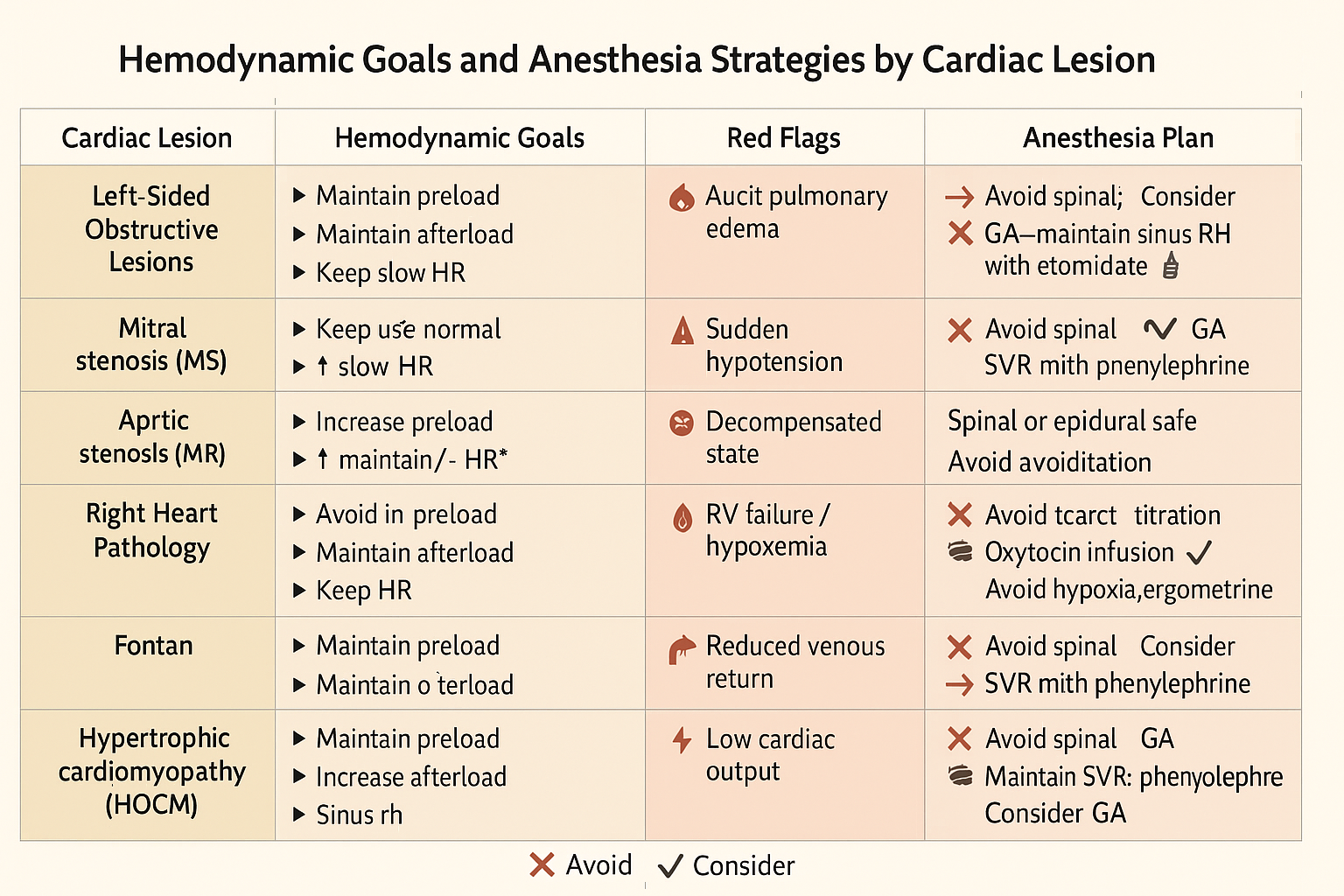
| Lesion Type | Preload | Afterload | Heart Rate | Rhythm | Key Risk |
|---|---|---|---|---|---|
| Stenosis (MS/AS) | Maintain | Maintain↑ | Low-normal | Sinus crucial | Fixed output – cannot increase CO |
| Regurg (MR/AR) | ↑ Preload | ↓ Afterload | ↑ HR (mod.) | Tolerates AF | Forward flow depends on low SVR |
| PHTN | Avoid ↑ | Maintain | Normal | Sinus helpful | Right heart failure, death post-delivery |
| HOCM | Maintain | ↑ Afterload | Low HR | Sinus critical | Outflow obstruction with ↓ preload |
| Mechanical valve | Maintain | Maintain | Avoid ↑ HR | Anticoagulate | Valve thrombosis, bleeding risk |
🔹 Left-Sided Obstructive Lesions
💔 Mitral Stenosis (MS)
- Common in rheumatic heart disease (especially in LMICs)
- Cannot accommodate ↑ preload → LAP ↑ → pulmonary edema
Hemodynamic Goals:
- Preload: Maintain
- Afterload: Maintain to slightly ↑
- HR: Keep <100 bpm to allow diastolic filling
- Rhythm: Sinus rhythm is critical
- Avoid: Fluid overload, tachycardia, aortocaval compression
Anesthetic Strategy:
- Epidural over spinal — gradual sympathectomy preferred
- GA: Use etomidate, avoid ketamine, maintain slow HR
- Phenylephrine preferred over ephedrine
Red Flag: Sudden dyspnea, orthopnea, pink frothy sputum = pulmonary edema
→ Give furosemide, morphine, sit up, O₂, urgent echo
💔 Aortic Stenosis (AS)
- Less tolerant of pregnancy than MS
- Fixed CO, at risk of sudden collapse during anesthesia
Hemodynamic Goals:
- Preload: Keep normal
- Afterload: ↑ (Avoid ↓ SVR)
- HR: 60–70 bpm
- Rhythm: Sinus — no atrial kick = disaster
- Avoid: Neuraxial-induced hypotension
Anesthetic Strategy:
- GA often safer
- Use etomidate, slow induction
- Maintain BP with phenylephrine
Clinical Tip: A spinal can be fatal in undiagnosed critical AS.
🔸 Left-Sided Regurgitant Lesions
💧 Mitral Regurgitation (MR) and Aortic Regurgitation (AR)
- Tolerate pregnancy well if compensated
- Forward flow improves with ↓ afterload
Hemodynamic Goals:
- Preload: Slightly ↑
- Afterload: ↓ (keep SVR low)
- HR: Slightly ↑
- Rhythm: AF tolerated
Anesthetic Strategy:
- Spinal or epidural are both safe if hemodynamically stable
- Avoid excessive vasoconstriction (Phenylephrine in small titrated doses)
- Maintain fast-smooth induction
Clinical Tip: In decompensated MR, high left atrial pressure mimics mitral stenosis.
🔺 Right Heart Pathology
🫁 Pulmonary Hypertension (PHTN)
- Pregnancy often contraindicated
- Most fatal during labor/postpartum from RV failure or PE
Hemodynamic Goals:
- Preload: Maintain
- Afterload: Don’t increase PVR!
- HR: Avoid tachycardia
- Rhythm: Keep sinus
Avoid:
- Hypoxia
- Hypercarbia
- Acidosis
- High PEEP
- Ergometrine / PGF2α (↑ PVR!)
Anesthetic Strategy:
- Epidural with slow titration
- Avoid GA if possible
- Oxytocin by infusion only
- Misoprostol is safe
🫀 Ebstein Anomaly
- Associated with tricuspid regurgitation, right atrial enlargement
- Prone to arrhythmias
Strategy:
- Avoid air embolism
- Care with oxytocin bolus
- Monitor arrhythmias; keep K⁺, Mg²⁺ normal
- Regional anesthesia is usually tolerated
🧬 Congenital Disease: TOF, Fontan, Eisenmenger
🔹 Repaired Tetralogy of Fallot (TOF)
- Often NYHA I–II
- Watch for RV dysfunction or arrhythmias
🔹 Fontan Circulation
- Preload dependent, NO pulmonary pump
- Fixed CO
- Avoid hypotension, diuresis, or high PEEP
- Maintain rhythm and venous return
- Avoid spinal anesthesia — epidural/GA better
🔺 Eisenmenger Syndrome (Class IV - Contraindicated)
- Right-to-left shunt
- Pregnancy = unacceptably high mortality
Never allow hypotension
Avoid high FiO₂ + PEEP combo
Monitor closely, delivery in ICU/OR suite
⚙️ Mechanical Heart Valves & Systemic Right Ventricle
🛠️ Mechanical Valve
- Anticoagulation is the key dilemma
| Trimester | Anticoagulation Strategy |
|---|---|
| 1st | LMWH or low-dose warfarin (<5 mg) |
| 2nd | Warfarin if safe, else LMWH with anti-Xa |
| 3rd | Switch to LMWH before labor, then UFH if surgery expected |
Neuraxial: Delay ≥24h after LMWH (therapeutic), 4–6h after UFH
Delivery: Avoid instrumental unless INR/anti-Xa acceptable
🔄 Systemic RV (e.g., Congenitally corrected TGA)
- Ventricular dysfunction and arrhythmia risk
- Plan early referral and close surveillance
💣 Hypertrophic Cardiomyopathy (HOCM) & Peripartum Cardiomyopathy (PPCM)
🧱 HOCM
- Dynamic outflow obstruction
- Worsens with ↓ preload, ↓ afterload, ↑ HR
Strategy:
- Avoid spinal → use GA or epidural
- Use phenylephrine (↑ SVR)
- Keep HR slow
- Keep well hydrated
🧨 Peripartum Cardiomyopathy
- Presents late pregnancy or postpartum
- EF <45%, risk of arrhythmias and thromboembolism
Management:
- Diuretics, vasodilators, beta blockers
- Avoid fluid overload
- Consider bromocriptine (inhibits prolactin)
- Cardiac MRI or echo before another pregnancy
⚡ Arrhythmias & Conduction Defects
- Pregnancy ↑ adrenergic tone → supraventricular arrhythmias common
- Treat sustained VT or AF with:
- Beta blockers (except atenolol)
- Amiodarone only if life-threatening
- Adenosine for AVNRT is safe
- Consider cardioversion if hemodynamically unstable
📌 Always check K⁺/Mg²⁺ before labor and surgery
📌 Consider loop recorder or telemetry for frequent episodes
🧠 Clinical Memory Map: “SWORD Your Strategy by Lesion”
- Stenosis → slow HR, sinus rhythm, stable SVR
- Wide regurg → want low SVR, higher HR
- Obstructive lesions → avoid neuraxial drop
- Right heart failure → avoid hypoxia, PEEP
- Decompensated cardiomyopathy → manage volume strictly
4️⃣ Pregnancy Heart Team & Preconception Counseling
Designing Safety Before the First Heartbeat
🧭 Why This Section Matters
Cardiac disease in pregnancy is rarely an acute surprise — it is predictable, preventable, and often manageable if addressed before conception.
When a woman with known or suspected heart disease is considering pregnancy, she deserves clarity, risk disclosure, and empowered decision-making.
This section defines how to build a cardio-obstetric team and what to cover in preconception counseling, especially in high-risk and limited-resource settings.
🤝 The Pregnancy Heart Team: Core Members & Roles
The cardio-obstetrics team is central to maternal safety. It should be activated in any patient with mWHO Class II–IV or when significant risk is suspected.
| Role | Responsibilities |
|---|---|
| Cardiologist | Diagnose and stratify risk, optimize medications, follow during pregnancy |
| Obstetrician (high-risk) | Plan delivery timing/location, monitor fetal growth and maternal symptoms |
| Anesthetist | Evaluate anesthesia options, prepare intrapartum/postpartum plans |
| Specialist midwife | Provide continuity, coordinate care, support patient education |
🧩 Optional members depending on case:
- Geneticist (inherited disease like Marfan, LQTS)
- Cardiac surgeon (severe lesions pre-surgery)
- Critical care team (for ICU/ventilatory support planning)
- Haematologist (anticoagulation management)
- Neonatologist (fetal risk, preterm risk)
- Social worker (complex psychosocial issues)
📌 ESC 2018 Guidelines recommend documentation of the care plan in patient notes and a copy provided to the patient — accessible 24/7.
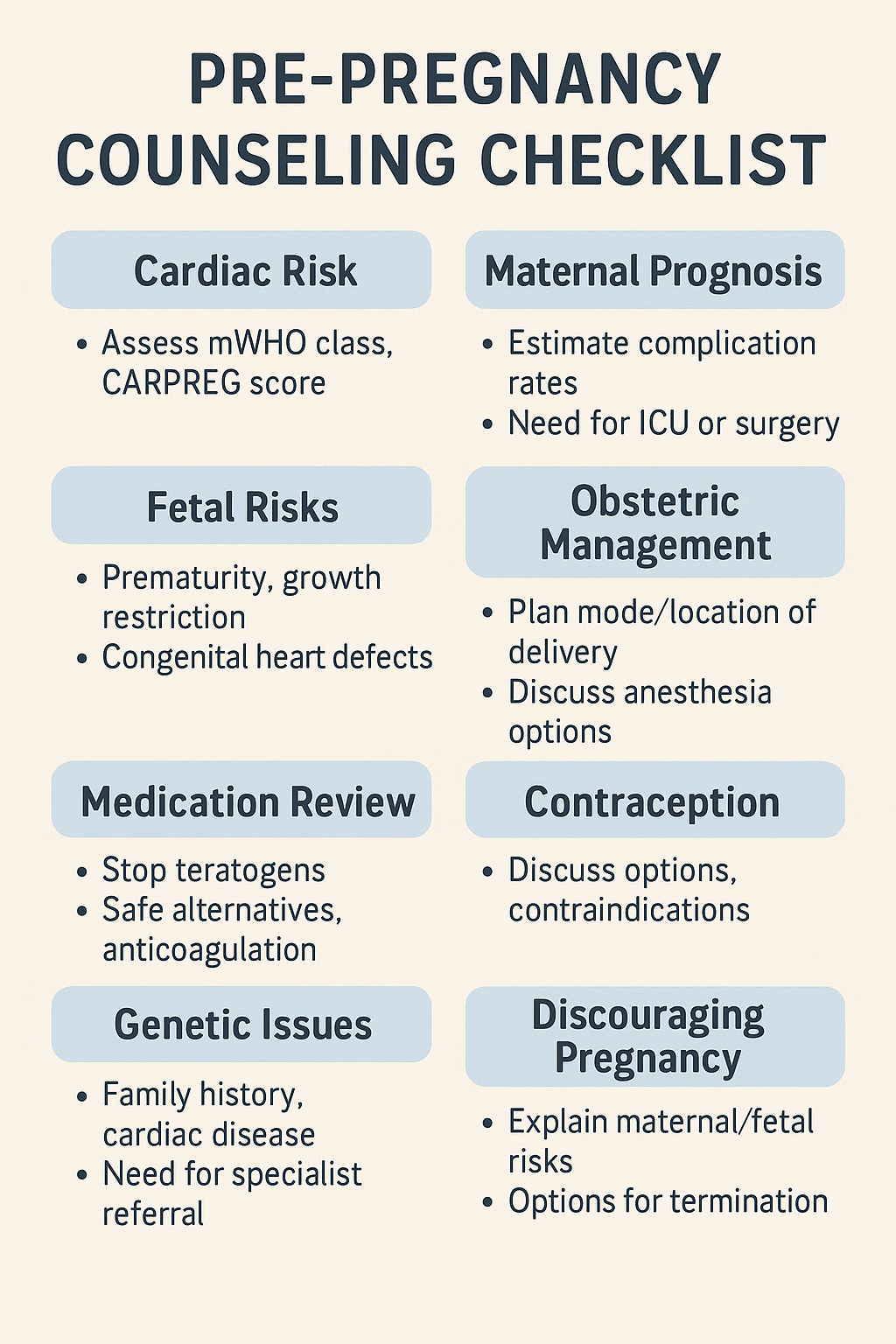
🧠 Key Elements of Preconception Counseling
| Domain | Content Covered |
|---|---|
| Cardiac Risk | mWHO class, CARPREG II score, previous ACE or surgery |
| Maternal Prognosis | Risk of heart failure, arrhythmia, need for ICU/ventilation |
| Fetal Prognosis | Risk of prematurity, growth restriction, hypoxia |
| Obstetric Strategy | Likely delivery mode, anesthesia approach, location of care |
| Medication Plan | Review teratogens, safe alternatives, anticoagulation plan |
| Emergency Scenarios | What happens if deterioration occurs during pregnancy or labor |
🧬 A woman must leave this session with either:
- An individualized pregnancy care plan, or
- A clear explanation of why pregnancy is not advised
⚠️ Counseling When Pregnancy Is Discouraged (mWHO IV)
Conditions where pregnancy should strongly be discouraged or terminated:
- Pulmonary arterial hypertension
- Severe mitral/aortic stenosis
- EF < 30% or NYHA III–IV
- Fontan circulation with cyanosis
- Eisenmenger syndrome
- Aortic dilation > 50 mm (>45 mm in Marfan)
- Mechanical valve with poor anticoagulation access
🩺 If a patient becomes pregnant:
- Early MDT counseling session
- Termination should be discussed compassionately but clearly
- If pregnancy continues, transition to Class III surveillance and tertiary care
💊 Contraception & Medication Review
Contraception must be offered to every woman at risk — especially if pregnancy poses significant mortality.
| Cardiac Risk | Preferred Contraception Options |
|---|---|
| High-risk EF < 30% | Levonorgestrel IUD, POP, barrier (avoid estrogen) |
| Warfarin users | Non-hormonal or progestin-only options preferred |
| Arrhythmia patients | Avoid estrogen (may provoke arrhythmias) |
| Pulmonary HTN | LARC methods preferred, avoid estrogen |
📌 Copper IUDs may provoke vasovagal syncope in some cardiac patients — insert under monitored conditions.
🧬 Genetic Counseling & Family History
- Assess for inherited syndromes:
- Marfan, Turner, LQTS, Brugada, HOCM
- Offer fetal echocardiography at 19–22 weeks
- Consider parental genetic testing if congenital or inherited risk is high
🧠 Involve the geneticist early if:
- Family history of sudden death < 50 yrs
- Syndromic features or connective tissue disorder
- Sibling with congenital cardiac anomaly
📌 Clinical Tip: Counseling = Precision Medicine
The goal is not to "scare" — but to clarify.
Let the patient know:
“Our job is to prepare for everything. The more we plan together, the more we protect you and your baby.”
5️⃣ Antenatal Assessment & Serial Investigations
Targeted Surveillance for Maternal-Fetal Safety
📍 Why This Section Matters
Many maternal cardiac complications can be predicted or prevented by focused surveillance. A missed murmur or skipped echo could mean decompensation in labor or loss in the postpartum period.
This section guides clinicians on:
- What to ask 🗣️
- What to test 🔬
- When to repeat 🗓️
- Where to refer 🏥
🩺 Targeted Cardiovascular History & Red Flags
Every visit must go beyond “How do you feel?”
These specific symptoms signal possible deterioration:
| Symptom | Concern to Rule Out |
|---|---|
| Orthopnea / PND | Pulmonary congestion (MS, PPCM) |
| Fatigue out of proportion | Low EF or fixed output lesion |
| Palpitations or syncope | Arrhythmia, aortic stenosis |
| Chest pain radiating to back | Aortic dissection (especially Marfan/Turner) |
| Hemoptysis / frothy sputum | Pulmonary edema in mitral stenosis |
| Resting HR > 120 bpm | Arrhythmia, decompensation |
| RR > 25/min or SpO₂ < 95% | Heart failure or pulmonary hypertension |
🧠 Always ask about:
- Prior cardiac surgery or interventions
- Family history of sudden death or cardiac disease
- Baseline exercise tolerance (pre-pregnancy)
🩻 ECG, NT-proBNP, and Functional Testing
📈 12-Lead ECG
- Baseline in all patients with risk
- Normal pregnancy changes:
- Left axis deviation (15–20°)
- Flattened or inverted T waves in III, V1–V2
- Q wave in III
🔍 Look for:
- New bundle branch blocks
- Atrial fibrillation
- QT prolongation (especially in LQTS)
🧪 NT-proBNP and Troponin
- BNP <100 pg/mL = strong negative predictive value for decompensation
- NT-proBNP >300–400 in pregnancy → suggestive of LV strain or failure
- Troponin only when ACS suspected; always correlate clinically
🧠 BNP can help distinguish dyspnea of pregnancy vs. cardiac cause
🏃 Stress Testing
- Safe before pregnancy only
- During pregnancy:
- Submaximal exercise testing for asymptomatic moderate-risk patients
- Use with caution — avoid in severe valve disease or arrhythmia history
🔍 Echocardiography: Gold Standard
🫀 Indications:
- Any known cardiac disease
- Any unexplained dyspnea, fatigue, or murmur
- Baseline echo by end of 1st trimester
- Repeat: each trimester or when symptoms evolve
| What to Monitor on Echo |
|---|
| Ejection fraction |
| Valve gradients (especially MS, AS) |
| Aortic root diameter |
| LV thickness (HOCM) |
| RV systolic pressure (PHTN suspicion) |
| Pericardial effusion in autoimmune disease |
📌 Transesophageal Echo can be used if needed in complex cases or poor transthoracic windows — it is safe in all trimesters.
🧲 Imaging Modalities in Pregnancy: What’s Safe?
| Modality | Use In Pregnancy | Notes |
|---|---|---|
| Chest X-ray (CXR) | Safe with abdominal shielding | For heart size, PHTN, pulmonary edema |
| CT Angiography | Safe when indicated | Use for PE, aortic dissection (if echo inconclusive) |
| MRI (non-contrast) | Safe in all trimesters | Ideal for congenital or structural assessment |
| MRI with Gadolinium | Avoid (esp. 1st trimester) | Only if benefit outweighs risk |
| Cardiac catheterization | Rarely used | If essential (e.g., coronary angiogram or ablation), use zero-fluoro or minimal-fluoro techniques |
📌 Always document risk/benefit and involve radiology + OB.
👶 Fetal Surveillance & Fetal Echo
🫀 Fetal Echocardiography (19–22 weeks):
- Indicated in:
- Maternal congenital heart disease
- Family history of CHD or sudden death
- Diabetic or lupus patients
- Medication exposure (e.g. lithium, valproate)
🩺 Growth Monitoring
- Monitor fetal growth every 4 weeks in:
- Cardiac lesions with ↓ uteroplacental flow (e.g. severe MS, PAH)
- Mothers on beta-blockers, anticoagulants
- Those with previous preterm or IUGR
📌 Umbilical artery doppler may help guide timing of delivery in FGR
🏥 Referral to Tertiary Cardio-Obstetric Centers
Refer if:
- mWHO Class II–IV
- CARPREG II score ≥2
- Severe valve disease or EF < 45%
- Fontan, PAH, HOCM, or cyanotic heart disease
- Need for anticoagulation during pregnancy
- Access to ICU, echo, urgent intervention not available locally
🧠 Document the plan, including anesthesia strategy, backup center contacts, and drug protocols.
6️⃣ Labor & Delivery Planning
Where Strategy Becomes Survival
🕰️ Timing and Setting of Delivery
The decision of when and where to deliver is not merely logistical — it is life-preserving for both mother and fetus.
| Patient Risk Level | Recommended Setting | Timing Strategy |
|---|---|---|
| mWHO I–II, stable NYHA I–II | Local hospital with basic monitoring | Await spontaneous labor or elective induction |
| mWHO II–III or CARPREG ≥2 | Tertiary cardio-obstetric center | Plan delivery by 39–40 weeks |
| mWHO III–IV or unstable | ICU-accessible OR with 24/7 multidisciplinary team | Elective delivery at 37–38 weeks, or earlier if decompensated |
📌 Always schedule delivery in daylight hours, with full team availability, not weekends or on-call gaps.
🧭 Vaginal vs. Cesarean Delivery — Not a Matter of Preference
| Mode | When Preferred | Benefits |
|---|---|---|
| Vaginal | Most stable lesions (regurgitation, mild MS) | Less blood loss, lower infection, better recovery |
| Cesarean | For cardiac indications, not just obstetric: | Controlled hemodynamics, avoids Valsalva, avoids labor strain |
| - Severe MS or AS | ||
| - PAH or Eisenmenger | ||
| - Mechanical valve on warfarin | ||
| - Aortic aneurysm >45 mm (or >40 mm in Marfan) | ||
| - Recent cardiac decompensation |
Induction of labor is safer than spontaneous labor in most high-risk cardiac patients.
🧪 Safe Induction of Labor in High-Risk Patients
| Method | Considerations |
|---|---|
| Foley balloon | Safe, mechanical method; no systemic vasodilation |
| Oxytocin | Use as infusion only; bolus can drop SVR rapidly |
| Misoprostol (PGE1) | Safe for most; rectal or sublingual routes preferred |
| Prostaglandin F2α | Avoid in PHTN or RV dysfunction — increases PVR |
| Ergometrine | Use only when necessary; avoid in AS, PHTN, IHD |
🧠 Always preload strategy before induction:
- CVP line in Fontan
- Strict fluid balance in cardiomyopathy
- Cardiac output monitoring in PAH
🩺 Invasive Monitoring: Use It Wisely
| Monitor | When Indicated |
|---|---|
| Arterial Line | Class III–IV lesions, fixed output (AS/MS), severe PHTN, vasoactive use |
| CVP Line | Fontan circulation, RV failure, HOCM with diuresis |
| Cardiac Output Monitor | PAH, EF <30%, perioperative decompensation |
| Pulse Oximetry + ECG | Minimum standard for every patient with mWHO II–IV risk |
📌 Avoid central lines in coagulopathy or full-dose anticoagulation without hematology input.
🤝 Coordinating with ICU, HDU, Neonatology — A Non-Negotiable Alliance
All high-risk patients must be booked into a unit with:
✅ Access to:
- ICU/HDU bed post-delivery
- Cardiologist on-call
- Anesthesia consultant experienced in cardiac disease
- Blood bank readiness (esp. for anticoagulated patients)
✅ Intra-delivery roles:
- Neonatologist in delivery room if fetal compromise is possible
- Obstetric anesthetist to manage GA or neuraxial challenges
- Echo machine ready for intra/postpartum cardiac deterioration
- Code protocol visible for cardiac arrest in pregnancy (per ACLS-modified)
🧠 Clinical Insight: What Fails Patients in Real Life?
🔻 Not timing delivery → Labor starts at 3 a.m. in a local clinic
🔻 Bolus of oxytocin → Hypotension → arrest in AS patient
🔻 No plan for INR reversal → bleeding after cesarean
🔻 Neonatal team not present → asphyxia in known IUGR
👉 All of these are avoidable with structured delivery planning.
📌 Quick Summary Table: Labor Delivery Logic by Risk Level
| Risk Level | Mode | Location | Special Needs |
|---|---|---|---|
| mWHO I–II | Vaginal | Local or secondary care | ECG, epidural, fetal monitoring |
| mWHO II–III | Vaginal/CS | Tertiary center | Arterial line, planned induction, anesthetist |
| mWHO IV | CS | Tertiary + ICU access | ICU bed, blood products, full MDT at bedside |
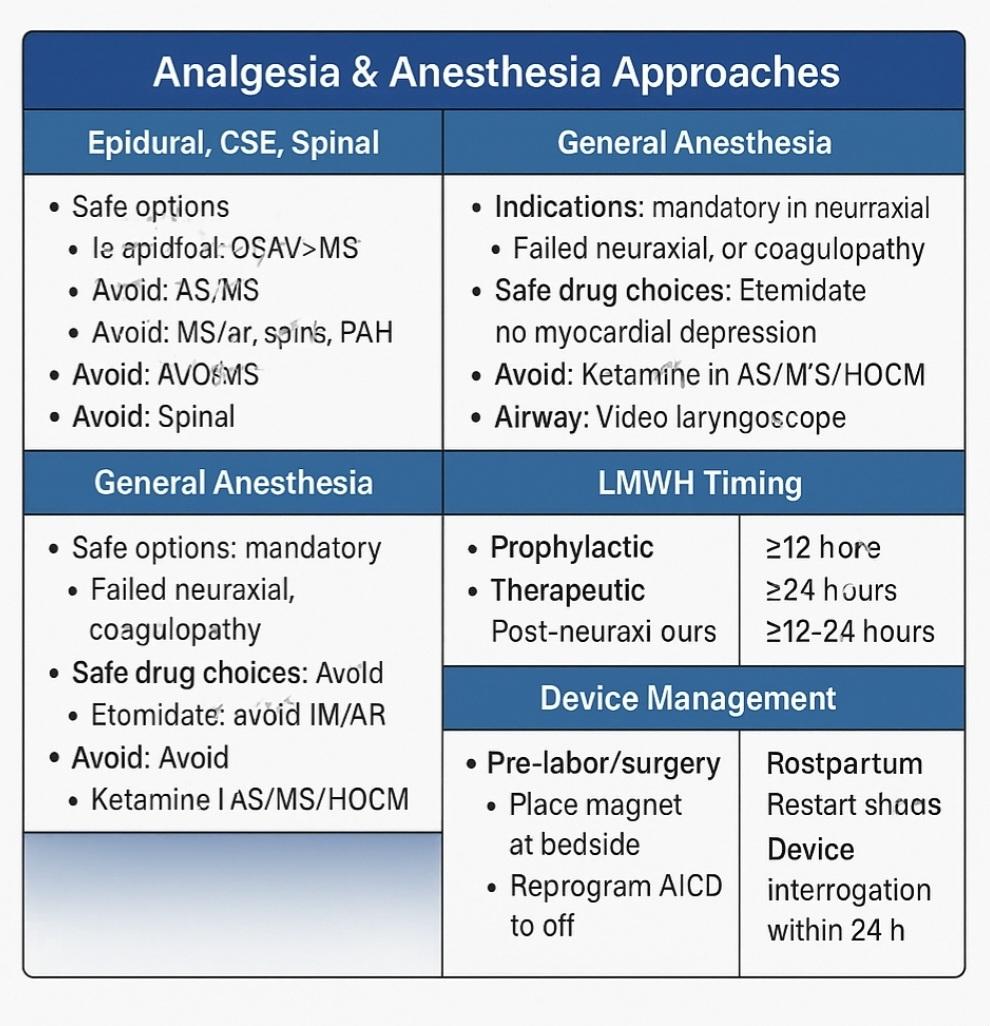
7️⃣ Analgesia & Anesthesia Approaches
Neuraxial, General, and Pharmacologic Strategy in Cardiac Pregnancy
⚖️ Core Principle: Match the Technique to the Lesion
Every cardiac lesion carries a hemodynamic signature — and anesthesia must be tailored to preserve that balance.
| Technique | Best For | Caution / Contraindicated In |
|---|---|---|
| Epidural | Most stable lesions (MR/AR, mild MS) | Severe AS/MS if bolused rapidly |
| CSE | Select cases needing fast-onset but titratable | AS, Fontan, severe cardiomyopathy |
| Spinal | Stable lesions only — avoid in fixed output | Severe MS/AS, HOCM, PAH, Eisenmenger |
| GA | Severe lesions, failed neuraxial, coagulopathy | High PEEP risk in PHTN, laryngoscopy-induced tachycardia |
🧵 Neuraxial Anesthesia — The Gold (But Not Always Safe) Standard
📌 Epidural
- Preferred in mWHO II–III, slow onset, adjustable
- Allows labor analgesia and conversion to anesthesia
- Maintain SVR with phenylephrine infusion
- Avoid bolus doses in stenotic lesions
⚠️ CSE (Combined Spinal-Epidural)
- Offers faster onset with backup control
- Only safe if:
- EF > 45%, no PHTN
- Preload can tolerate rapid vasodilation
🚫 Spinal Alone
- Avoid in:
- Severe MS/AS, PHTN, Eisenmenger, Fontan, EF < 30%
- Sudden drop in SVR → reflex tachycardia → ischemia/arrhythmia
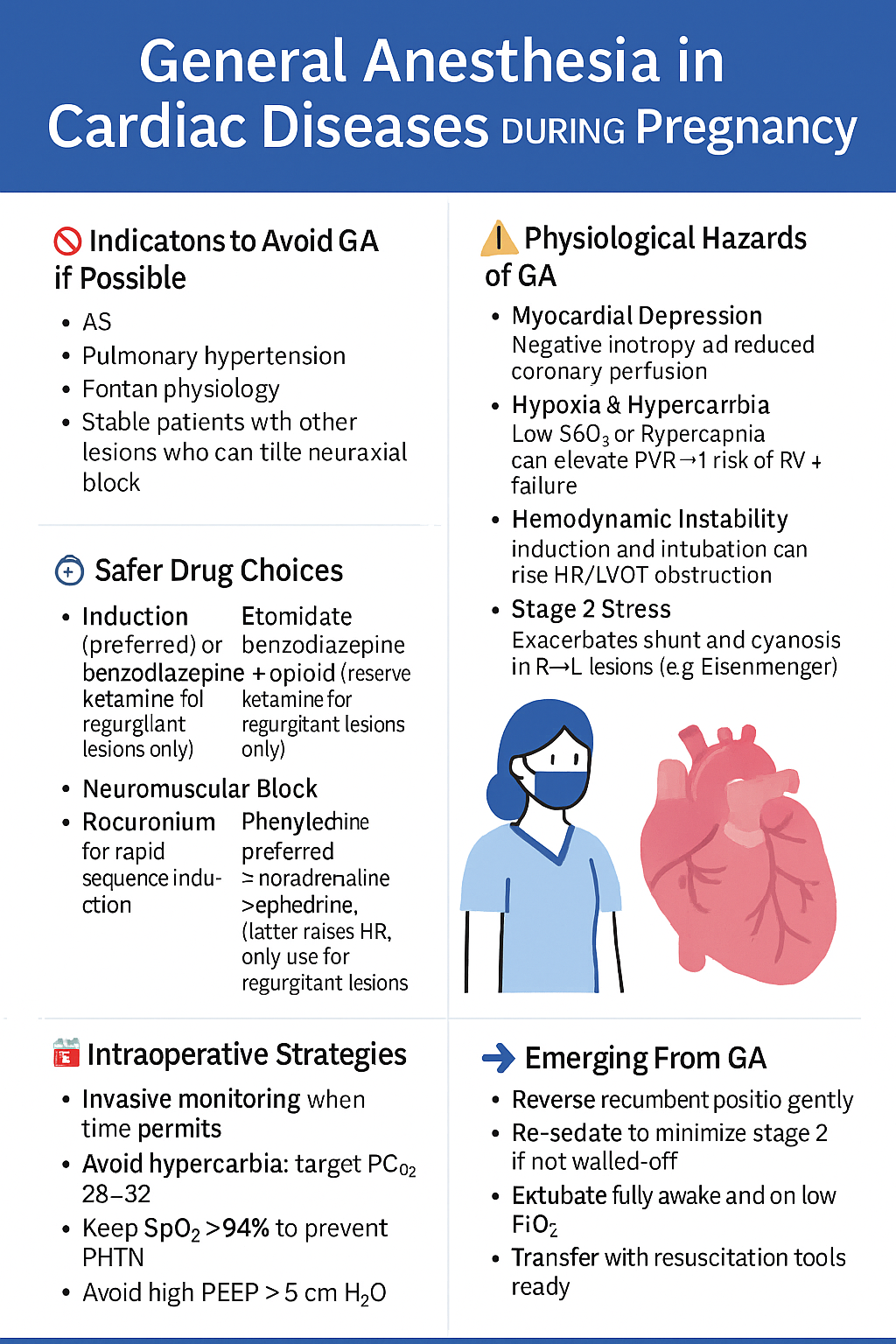
💤 General Anesthesia — When It Is Mandatory
| Indications |
|---|
| Failed/contraindicated neuraxial technique (coagulopathy, LMWH timing) |
| Severe aortic stenosis, HOCM, or uncooperative unstable patient |
| Emergency Cesarean with no time for epidural dosing |
| Airway risk + cardiac lesion needing precise hemodynamics |
🔐 Induction Plan
- Etomidate: Best in low EF, no myocardial depression
- Propofol: Caution — can drop SVR (safe in MR/AR only)
- Ketamine: Avoid in MS, AS, HOCM (↑ HR and contractility = disaster)
- Opioids: Use judiciously (fentanyl or remifentanil)
🌬️ Airway & Ventilation
- Use video laryngoscopy (avoid prolonged laryngoscopy)
- Preoxygenate carefully
- Minimize PEEP in PHTN and RV dysfunction
- Avoid hypercapnia or hypoxia — can precipitate arrhythmia or vasoconstriction
💉 Vasopressors: Choose Wisely
| Drug | Action | Use in: | Avoid in: |
|---|---|---|---|
| Phenylephrine | ↑ SVR, reflex ↓ HR | MS, AS, HOCM | Severe bradycardia |
| Ephedrine | ↑ HR and contractility | MR/AR, spinal-induced hypotension | AS, HOCM, ischemic heart |
| Metaraminol | Mild alpha + beta | Good alternative in GA | Severe PHTN |
📌 Start vasopressors early in neuraxial — don’t wait for hypotension.
⏰ Timing of LMWH and Neuraxial Techniques
| LMWH Dose Type | Minimum Delay Before Neuraxial | After Neuraxial → Restart Time |
|---|---|---|
| Prophylactic | ≥12 hours | ≥4 hours post-procedure |
| Therapeutic | ≥24 hours | ≥12–24 hours post-op (esp. with PPH) |
| UFH IV | 4–6 hours | 1 hour after catheter removal |
🧠 Always consult hematology in mechanical valve or HIT cases.
⚙️ Pacemakers & Implantable Cardioverter-Defibrillators (AICDs)
💡 Before Labor / Surgery:
- Confirm device function & settings
- Place magnet at bedside
- If delivery imminent, reprogram ICD to off during cesarean or GA
- Avoid monopolar diathermy; use bipolar or short bursts
⚠️ Postpartum:
- Device interrogation within 24 hours
- Restore defibrillator functions if turned off
📌 Always place external defibrillator pads before GA or regional in patients with an AICD.
🧠 Clinical Gems to Remember
✅ Epidural is best when titrated slowly in most lesions
✅ Spinal can kill in MS/AS/PAH — avoid it
✅ Etomidate is the safest induction agent for low EF or stenosis
✅ Ketamine = red flag for HOCM, MS, AS
✅ Don't push oxytocin as a bolus — infuse slowly in all patients
✅ Always consider fetal bradycardia when mother becomes hypotensive
8️⃣ Pharmacology, Anticoagulation, and Uterotonics
Medications That Save — or Sabotage — the Cardiac Pregnancy
💊 Safe & Unsafe Cardiovascular Drugs in Pregnancy
| Drug Class | Safe to Use in Pregnancy | Avoid or Use With Caution |
|---|---|---|
| Beta-blockers | Labetalol, Metoprolol, Bisoprolol | Atenolol → IUGR risk |
| Diuretics | Furosemide (low dose), spironolactone (later) | High-dose loops → ↓ placental perfusion |
| Calcium channel blockers | Nifedipine (HTN), Diltiazem (arrhythmia) | Verapamil in 3rd trimester (↑ uterine tone) |
| ACEi / ARBs | ❌ CONTRAINDICATED — teratogenic | Avoid in all trimesters |
| Amiodarone | ❌ Use only for life-threatening arrhythmia | Thyroid dysfunction in fetus/neonate |
| Digoxin | Can be used safely for rate control | Monitor levels closely — may cross placenta |
| Statins | ❌ Teratogenic — contraindicated | Stop pre-pregnancy if on them |
| Nitrates | Yes — for preload reduction, angina | Watch BP in severe AS or preload-dependent states |
⚖️ Anticoagulation Strategy Across Trimesters
📌 Indications for Anticoagulation
- Mechanical heart valve
- Atrial fibrillation with CHADS2-VASc ≥2
- History of thromboembolism
- Severe LV dysfunction (EF <30%)
- Known thrombophilia (antiphospholipid, protein C/S deficiency)
🩸 Trimester-Specific Anticoagulant Strategy
| Trimester | Preferred Strategy |
|---|---|
| 1st | LMWH preferred (start therapeutic dosing) |
| Consider warfarin if low-dose <5 mg/day (less teratogenic) | |
| 2nd | Warfarin if required — less risk of embryopathy |
| LMWH with anti-Xa monitoring if warfarin not feasible | |
| 3rd | Switch to UFH or LMWH before planned delivery |
| Goal: avoid neuraxial bleeding and ensure rapid reversal |
📌 Bridging LMWH → UFH at 36 weeks if Cesarean planned
📌 Stop UFH 4–6h before neuraxial block; resume ≥6h after
🧪 Monitoring Parameters
- LMWH: Check anti-Xa level 4–6 hours post-dose
- Target: 0.6–1.0 IU/mL (therapeutic), 0.2–0.6 (prophylactic)
- Warfarin: Maintain INR 2.5–3.5 for mechanical valves
- UFH: aPTT 1.5–2.5× control
🧠 Always repeat platelet count to exclude HIT if on heparin >4 days.
🚫 Direct Oral Anticoagulants (DOACs) in Pregnancy
| Drug | Status |
|---|---|
| Rivaroxaban, Apixaban, Dabigatran | ❌ NOT safe — avoid in all trimesters and lactation |
| Edoxaban | ❌ Limited data, not recommended |
🤱 Breastfeeding Considerations
| Drug | Safe in Breastfeeding? |
|---|---|
| Warfarin | ✅ Yes — does not enter breast milk |
| LMWH / UFH | ✅ Yes — large molecules |
| Aspirin (low dose) | ✅ Yes |
| Clopidogrel | ⚠️ Use caution — limited data |
| Amiodarone | ❌ Avoid — accumulates in infant |
🧬 Uterotonic Agents — Cardiovascular Effects
| Agent | Effect on Hemodynamics | Use With Caution In… |
|---|---|---|
| Oxytocin (bolus) | ↓ SVR → reflex tachycardia, hypotension | MS, AS, HOCM, fixed output lesions |
| Oxytocin (infusion) | Safe when titrated slowly | Preferred method in all cardiac cases |
| Ergometrine | ↑ SVR + ↑ PVR → hypertension, arrhythmia, vasospasm | AS, PHTN, ischemic heart disease |
| Misoprostol | Minimal effect on SVR — safe | Use rectally or sublingually |
| PGF2α (Carboprost) | ↑ PVR, bronchospasm, hypoxia | Avoid in PAH, RV failure, Fontan |
📌 Always document dose and route. Oxytocin should be started as an infusion (e.g., 5 IU in 500 mL over 3–4h).
🧠 Clinical Insights for Pharmacology in Pregnancy
✅ Start LMWH early in mechanical valves — don’t delay
✅ Always document last anticoagulant dose in laboring patients
✅ Use phenylephrine to maintain SVR, not ephedrine, in fixed lesions
✅ Avoid oxytocin bolus, use infusion only
✅ Ergometrine should be written "avoid unless hemorrhage" in the anesthesia plan
9️⃣ Postpartum Surveillance & Complications
Where Most Maternal Deaths Hide — and How to Prevent Them
🚨 Why This Section Is Critical
The postpartum period — especially the first 24–48 hours — is when the majority of cardiac maternal deaths occur.
Why? Because after delivery:
- Venous return spikes from uterine autotransfusion
- SVR rebounds, worsening stenotic and cardiomyopathic states
- Fluid mismanagement, late anticoagulation, or missed arrhythmia can be fatal
This is not the time to relax — it’s when we must monitor like intensivists and plan like generals.
🛏️ Who Needs ICU/HDU for Postpartum Monitoring?
| Condition or Lesion | Recommended Level of Care |
|---|---|
| Severe MS, AS, HOCM | ICU or HDU × 48 hours |
| Fontan physiology, PHTN, Eisenmenger | ICU mandatory |
| EF < 30%, PPCM, decompensated cardiomyopathy | ICU with echo and inotrope backup |
| Mechanical valve with anticoagulation | HDU for bleeding/thrombosis risk |
| Recent arrhythmia, syncope, or VT/VF | ICU with telemetry |
📌 Minimum for all mWHO III–IV:
- Continuous ECG
- Strict input/output
- 4–6 hourly vitals
- Oxygen and furosemide at bedside
🌊 Recognizing Flash Pulmonary Edema
⏱️ Usually occurs within 1–4 hours after delivery, as:
- Uterine contraction autotransfuses ~500 mL
- SVR increases as placenta separates
- Diastolic dysfunction or mitral stenosis causes LA pressure surge
🚨 Warning Signs:
- Sudden dyspnea, orthopnea
- Pink frothy sputum
- Tachypnea, SpO₂ drop
- New S₃ or crepitations
📌 Immediate Actions:
- Sit up, give oxygen
- Administer IV furosemide 20–40 mg
- Morphine if anxious/hypertensive
- STAT echo if not recently done
- Call cardiology + ICU if not already present
🩸 Restarting Anticoagulation Post-Delivery
| Drug | Restart Timing* |
|---|---|
| LMWH (prophylactic) | ≥ 4–6 hours after vaginal/cesarean delivery (if no bleeding) |
| LMWH (therapeutic) | ≥ 12–24 hours post-delivery, depending on blood loss |
| UFH IV | After epidural removal + ≥1h |
| Warfarin | Restart 12–24 hours post-delivery (monitor INR) |
*Always involve hematology in mechanical valve patients.
💊 Postpartum Pain Control: Safe Choices
| Drug Class | Safe in Cardiac Patients? | Notes |
|---|---|---|
| Paracetamol | ✅ Yes | First-line, minimal interaction |
| NSAIDs | ⚠️ Use cautiously | Avoid if CHF, renal dysfunction, or full anticoagulation |
| Opioids | ✅ In moderation | IV morphine or oral tramadol ok |
| Regional Block | ✅ (if no anticoagulation yet) | TAP block, wound infiltration |
🤱 Breastfeeding Considerations for Cardiac Meds
| Medication | Safe in Breastfeeding? | Notes |
|---|---|---|
| Warfarin | ✅ Yes | Does not cross into breast milk |
| LMWH / UFH | ✅ Yes | Large molecules, non-transferred |
| Beta-blockers (labetalol, metoprolol) | ✅ Yes | Monitor infant HR |
| ACEi (enalapril, captopril) | ✅ Yes (with caution) | Avoid other ACEi |
| Amiodarone | ❌ No | Long half-life, risk to thyroid |
| Clopidogrel | ⚠️ Caution | Limited data — weigh risks |
📋 Discharge Planning & Long-Term Follow-Up
-
Discharge Summary should include:
- mWHO class
- Final echo findings
- Anticoagulation plan (drug + target INR or anti-Xa)
- Planned outpatient follow-up (cardiology, obstetrics)
-
Outpatient Plan:
- Cardiology visit in 2–4 weeks post-delivery
- Echo repeat at 6 weeks postpartum
- Contraception counseling (per previous lesion risk)
- Genetic screening follow-up if congenital
-
Emergency Instructions:
- Red flag symptom card provided
- When to go directly to ER (dyspnea, chest pain, syncope)
🧠 Patients discharged without education are at higher risk for readmission and maternal death.
🧠 Clinical Pearl
Most maternal cardiac deaths don’t happen in the OR.
They happen after discharge, in silence.
📌 Don’t stop at the surgery — plan for survival after delivery.
🔟 Resource-Limited Strategies
When the Stethoscope is Your Echo, and Judgement is Your ICU
🧭 Why This Section Matters
Not every patient delivers in a tertiary hospital with on-call cardiologists, echo techs, or immediate ICU access.
Yet cardiac disease doesn’t pause for infrastructure — it shows up in dusty clinics, midnight emergencies, and power outages.
This section teaches how to recognize, plan, and act — when tech fails, but training prevails.
👂 Clinical Assessment Without Echo or Biomarkers
✅ What to Rely On:
-
Symptoms:
- Orthopnea, PND, unexplained fatigue → suspect MS or PPCM
- Exertional syncope → suspect AS
- Palpitations with exertion → consider arrhythmia or RV strain
-
Vitals:
- Tachypnea > 22 → red flag
- HR > 110 at rest → not just “anxiety”
- SpO₂ < 95% on air → investigate further
-
Neck veins & pedal edema:
- Raised JVP, hepatomegaly, ascites → suggest RV failure or PHTN
🩺 How to Predict Lesion Severity With Auscultation
| Murmur | Likely Lesion | Clues to Severity |
|---|---|---|
| Mid-diastolic, apex | Mitral stenosis | Loud S1, opening snap, parasternal heave |
| Harsh systolic, aortic area | Aortic stenosis | Radiates to neck, slow-rising pulse |
| Pansystolic at apex | Mitral regurgitation | Radiates to axilla, soft S1 |
| Early diastolic at base | Aortic regurgitation | Bounding pulse, wide pulse pressure |
| Holosystolic LLSB | Tricuspid regurg or VSD | ↑ with inspiration (Carvallo sign) |
🧠 If murmur is new, loud, or associated with symptoms — treat it as dangerous until proven otherwise.
💉 Adapting Anesthesia Without ICU or Backup
✅ Safer Practices:
| Situation | Safer Adaptation |
|---|---|
| No ICU post-op | Use epidural with slow titration — avoid spinal in stenosis |
| No Etomidate available | Use ketamine only in regurgitant lesions — avoid in AS, MS, HOCM |
| No CVP or echo | Rely on fluid responsiveness and auscultation |
| No infusion pumps | Manually titrate vasopressors (phenylephrine best) |
| No blood gas machine | Use respiratory rate, SpO₂, mental status as surrogate |
📌 Always have furosemide, oxygen, and suction at bedside before labor starts in high-risk patients.
💊 Prioritizing Drug Availability
| Class | If You Have Only One Option | What to Do |
|---|---|---|
| Vasopressor | Phenylephrine | Titrate slowly via IV push |
| Induction | Ketamine (only if no stenosis present) | Give midazolam premed, small dose, slow titration |
| Anticoagulant | LMWH (avoid warfarin if no INR access) | Stick to therapeutic dosing by weight |
| Analgesia | Morphine or tramadol | Use lowest effective dose; combine with paracetamol |
🧠 If no metaraminol, ephedrine can be used — but be very cautious in stenotic or ischemic lesions.
🧳 Emergency C-Section in a District Hospital
Prepare Like This:
- Airway: Ensure backup blade, suction, mask seal
- IV Access: Two working 18G lines — flush ready
- Monitoring: BP cuff, SpO₂, ECG if possible
- Anesthesia: If patient is unstable — GA with etomidate or ketamine (regurg only)
- Fluid: Start warmed RL slowly — no routine bolus
- Uterotonics: Misoprostol or oxytocin by infusion only — no bolus
- Team: Assign 1 person to watch vitals, 1 for baby, 1 for meds
- Defibrillator: If none, prep external CPR access (chest clear)
🧠 Final Wisdom From Low-Resource Settings
“You don’t need machines to be safe — you need vigilance, calm hands, and the humility to listen to what the body tells you.”
1️⃣1️⃣ MCQs: High-Level Clinical Scenarios in Cardiac Disease & Pregnancy
Each question includes a brief rationale for immediate learning
1. Mitral Stenosis in Labor
A 28-year-old woman with known moderate mitral stenosis (mWHO III) presents in labor. Her HR is 112 bpm, RR 26, and she reports new-onset orthopnea. What is the most appropriate next step?
A. Administer IV fluids to improve preload
B. Begin slow epidural analgesia
C. Give IV furosemide and sit her upright
D. Start oxytocin bolus to expedite delivery
✅ Answer: C — Pulmonary edema is likely. Fluids would worsen. Epidural can come later.
2. Aortic Stenosis Induction
A woman with critical aortic stenosis needs a C-section for fetal distress. She is hemodynamically stable. Which induction agent is preferred?
A. Ketamine
B. Propofol
C. Etomidate
D. Midazolam
✅ Answer: C — Etomidate provides stability in fixed-output lesions. Ketamine worsens obstruction.
3. LMWH Timing Dilemma
A 32-year-old woman with mechanical mitral valve received her last therapeutic LMWH dose 14 hours ago. She now requires urgent C-section. What’s the safest approach?
A. Proceed with spinal anesthesia
B. Delay surgery until 24 hours passed
C. Convert to GA with careful airway control
D. Give protamine and proceed with epidural
✅ Answer: C — Neuraxial is contraindicated with therapeutic LMWH <24h. GA is safest.
4. Postpartum Arrhythmia
A postpartum patient with repaired TOF develops palpitations and HR 145 bpm. SpO₂ 95%. What is the most appropriate management?
A. Amiodarone IV
B. Adenosine IV push
C. Beta-blocker oral
D. Cardioversion
✅ Answer: B — Likely SVT. Adenosine is first-line and safe. Amiodarone is reserved for unstable cases.
5. Cardiomyopathy on Table
During C-section under GA, a woman with peripartum cardiomyopathy develops hypotension. Which vasopressor is preferred?
A. Ephedrine
B. Phenylephrine
C. Dopamine
D. Noradrenaline
✅ Answer: B — Maintain SVR without ↑ HR. Ephedrine can worsen tachycardia and reduce diastolic filling.
6. Oxytocin Use in MS
In a woman with severe MS, what’s the safest uterotonic strategy?
A. IV bolus oxytocin
B. Intramuscular ergometrine
C. Oxytocin infusion at 5 IU/hour
D. PGF2α rectally
✅ Answer: C — Slow oxytocin infusion avoids abrupt SVR drop.
7. AICD During Labor
A woman with an implanted AICD is in labor and requests an epidural. What’s the safest plan?
A. Turn off device before epidural
B. Leave device on, avoid diathermy
C. Only allow vaginal delivery under GA
D. Keep defibrillator off unless arrhythmia occurs
✅ Answer: B — Do not turn off the device unless using monopolar cautery. Have a magnet & external defib ready.
8. Fontan Circulation Monitoring
Which parameter is most critical in monitoring a laboring woman with Fontan physiology?
A. Urine output
B. Oxygen saturation
C. Central venous pressure
D. ECG rhythm
✅ Answer: C — Preload drives systemic circulation. CVP is the best guide.
9. Breastfeeding with Amiodarone
Which of the following is TRUE regarding amiodarone use postpartum?
A. Safe during breastfeeding
B. Preferred for AF control in lactation
C. Contraindicated due to fetal thyroid effects
D. Enhances milk production
✅ Answer: C — Accumulates in neonate. Avoid in breastfeeding mothers.
10. Eisenmenger in Labor
Which is most dangerous in a laboring woman with Eisenmenger syndrome?
A. Slow oxytocin infusion
B. Upright posture during 2nd stage
C. Hypoxia or hypercarbia
D. Epidural analgesia
✅ Answer: C — Anything that increases PVR (hypoxia/hypercarbia/acidosis) is life-threatening.
11. Misoprostol vs Ergometrine
Which uterotonic is safest in a woman with PHTN?
A. Misoprostol rectally
B. IV ergometrine
C. IV oxytocin bolus
D. PGF2α injection
✅ Answer: A — Misoprostol is safe. Ergometrine and PGF2α are dangerous in PHTN.
12. Timing of Postpartum Warfarin
When can warfarin be restarted safely after C-section?
A. 2 hours
B. 6 hours
C. 12–24 hours if no bleeding
D. Immediately post-delivery
✅ Answer: C — Delayed start reduces PPH risk, allows wound stability.
13. GA in AS Patient
A woman with severe AS is undergoing GA. Which is the biggest risk?
A. Tachycardia
B. Bradycardia
C. Increased contractility
D. High PEEP
✅ Answer: A — ↑ HR shortens diastole → ↓ coronary perfusion → ischemia.
14. Ephedrine Use in Labor
Ephedrine is contraindicated in which lesion?
A. Mitral regurgitation
B. Aortic regurgitation
C. Aortic stenosis
D. Tricuspid regurgitation
✅ Answer: C — Ephedrine ↑ HR and contractility → bad for fixed-output lesions like AS.
15. Emergency Cesarean in Remote Hospital
What’s the most important prep in a woman with known heart disease and no echo available?
A. IV antibiotics
B. Central venous line
C. Uterotonic preloading
D. Backup GA and resuscitation plan
✅ Answer: D — Prioritize airway, BP, resus tools. Uterotonics only after stable vitals.
🔚 Final Words: The Maternal Heart Under Pressure
In every delivery room, whether lit by halogen lights or kerosene lamps, there is one constant: the maternal heart carries two lives.
One beat, one decision, one drug — all can tilt the scale toward survival or loss.
This guide was not built just for exam scores or textbook shelves. It was shaped for:
- The anesthetist alone at night in a rural OR
- The junior doctor balancing risk without echo or labs
- The consultant rechecking ECGs before pushing a spinal dose
- And the pregnant woman who doesn’t yet know her heart carries risk
You’ve now seen how lesion-specific plans, tailored anesthesia, smart drug choices, and sharp observation can save lives — even when technology is absent.
We have equipped you to:
- Predict collapse before it happens
- Stratify risk with your mind, not just machines
- Deliver care confidently in tertiary centers and humble clinics alike
In cardiac disease, pregnancy is not just high-risk — it is high-stakes.
But risk can be managed. Outcomes can be changed.
And safety can be built — with vigilance, knowledge, and heart.
🧭 This guide is your reference when managing cardiac disease in pregnancy — in every setting.
Stay structured. Stay vigilant. Act wisely. 🧠
📌 Prepared for Dr. Amir Fadhel and Dr. Syed Zeeshan Javaid Hashmi – Specialists in Anesthesiology and Critical Care
🗓️ Created: 08/06/2025
🗓️ Last Updated: 08/06/2025
🔗 Explore the Full Mastery Series:
Mastery Series in Anesthesia & Critical Care