CAUTION: All of this is advice from non-professionals with no formal training on dosages, side effects, or other complications. We do not know about your specific medical circumstances, such as other medications you may be on or preexisting conditions. Be careful, do your own research, consult doctors first, and keep this in mind if following the advice here
(Updated version of https://pastebin.com/QCJEsu41)
Also consider looking into a pastebin originally from another author
>"What to do when Corona chan comes over to Netflix and Chill"
https://justpaste.it/87kdn
[Introductory tl;dr]
To give you a starting clue in the shortest way possible, for proper prophylactic and treatment measures, you will need anti-inflammatory and immunomodulating compunts, anti-oxidants, anticoagulants, as well as proper nutrition, plenty of vitamins (keep vitamin K, serum iron and calcium within strictly average levels though).
That applies for prophylaxis and treatment before taking the SARS-2 "vaccine products", and mitigation of any possible long-term complications from infection and/or the vaccines as well.
Table of contents (select the brackets and the word inside for CTRL+F search for detailed information and sources)
>[PROPHYLAXIS]
[Water] - ~3 liters per day
[Sleep] - ~8 hours per day
[Garlic] - thermally unprocessed, preferably crushed/cut ~10 minutes before consumption for maximum allicin formation (upper tolerable limit is ~11 cloves per day for an adult) (garlic pills, powder or supplements are a very subpar substitute due to lack of many nutrients and comparably limited formation of allicin)
[Zinc] - Up to 100 mg/day for prophylaxis purposes, up to 150 mg for treatment purposes
[Copper] - Up to 10 mg/day
[Green tea]
[Black tea]
[Catechins]
[N-Acetylcysteine] - 600 mg/day for prophylaxis, 1,200 mg/day for treatment
[Vitamin D] Up to 20,000 IU for prophylaxis purposes, up to 40,000 IU for treatment purposes
[Vitamin B (B3 (aka PP, aka niacin) especially)]
[Vitamin B12]
[Kvas (homemade)]
[Vitamin C] - at least 2000 mg/day for prophylaxis, and 3g every 3 hours for advanced prophylaxis or treament
[Nitric oxide or sources of L-arginine]
[L-serine]
[Sphingolipids]
[Lactoferrin] - at least 100mg for prophylactic purposes, at least 300mg for treatment purposes, non-supplement form is contained in dairy (0.174 g/l in low heat pasteurized cow’s milk (and 1.2 g/kg in semihard cheese produced from that milk)), maximum ~1.5g and ~3.5g for prophylactic and treatment purposes respectively
[Cheese]
[Carnitine]
[Anti-oxidants]
[Turmeric]
[Curcumin]
[Black pepper]
[Citrulline]
[Peppers]
[Capsaicin]
[Pelargonidin]
[Melatonin] - 1-10 mg for prophylaxis, 200 mg for treatment
[Honey]
[Nigella sativa]
[Propolis]
[Quercetin]
[Taurine, hypotaurine, homotaurine]
[Quinine]
[Bromelain]
[Probiotics]
[Gallic acid]
[Vitamin A]
[Vitamin E]
[Selenium]
[Magnesium]
[Carrot Pomace Polysaccharide]
[BONUS NOTES] (things to avoid or be aware of)
[Natural Killer cell enhancement]
[Blood-brain barrier (BBB) and blood-testis barrier (BTB) strengthening]
[Interfering with TMPRSS2 binding]
[Cathepsin L inhibitors]
[Pre-vaccination measures]
>[Secondary prophylaxis]
[Exercise]
[Gingerol]
[Mustard oil]
[Piperine]
[Nicotine patches]
[Cinnamon]
[Hop Extracts]
[Potassium]
[Etc]
[Exposure-specific prophylaxis and early-to-clearance treatment]
[Nattokinase] (from natto)
Nattokinase offers proteolytic degradation activity of SARS-CoV-2 proteins, would be also useful against SARS-2-Alzheimers and clots
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8276596
[Oral/nasal sprays]
[Iota-carrageenan spray]
[Nasal saline spray]
[Nitric oxide nasal sprays or supplements]
>[TREATMENTS]
>Continue with your diet and supplements listed above. Perhaps increase the dosage on the potent things, just absolutely do NOT overdose.
>Absolutely refrain from working out or straining your heart/body, let your body focus on dealing with the infection. It's a given even if you would be dealing with a flu or a common cold.
[steam inhalation]
[>OTC treatments]
[Blood thinners] (also mind your diet)
[Aspirin]
[Apixaban]
[Clopidrogel]
[Antihistamines (H1, H2)]
[Bismuth subsalicylate (Pepto-bismol)]
[Famotidine (Pepcid)]
[Nitric oxide nasal sprays, supplements or boosting sources]
[Methylene Blue]
[Naxproxen (Aleve)]
[Bromhexine]
[Colchicine]
[Ambroxol]
[Nasal saline spray]
[Niclosamide]
[Fenofibrate]
[Dexamethasone (6mg)]
[Inhaled corticosteroids]
[Nitazoxanide]
[>Unproven/fringe treatments]
[D-galactose supplements]
[Larazotide acetate]
[After clearance of the symptoms and the virus]
[smell training]
[Stimulation of neuronal growth/plasticity]
[intermittent fasting]
[Dealing with possible persistent mast cell activation]
[Mitigate and reverse demyelination]
[Anti-amyloid / misfolded protein disease / prion section]
[CONTRAINDICATIONS]
>[PROPHYLAXIS]
Things to do (aside from using proper PPE like a respirator with P3-tier filters and airtight protection of eyes) before becoming infected OR vaccinated, to reduce risks associated with infection/vaccination and/or improve potential outcome
Get an oximeter, monitor your oxygenation if you think/know you are infected, go to hospital or call your health care provider if your blood oxygenation drops below 95%, and consider calling an ambulance if it drops below 90%.
Mind that normal oxygen levels are at least 95%. Some patients with chronic lung disease or sleep apnea can have normal levels around 90%.
Use middle finger of dominant hand (or the three ring, index, middle according to other sources but not thumb or little finger) for the most accurate results for pulse oximetry.
Note that PI is also a good indicator of the reliability of the pulse oximeter reading. For most pulse oximeters for general use, the reading is unreliable or unavailable if PI is at or below 0.4%
>study find that home oximetry monitoring can be a safe pathway for Covid-19 patients; and indicates increases in risk to vulnerable groups and patients with oxygen saturations < 95% at enrolment, and in those enrolled on discharge from hospital
https://archive.vn/ZBk3Q
>proven/most critical/easiest
[Water]: Consume ~3 liters of water a day. This should be done as part of a healthy lifestyle, pandemic or not. Water is critical for immune and body function. If the disease gets severe, avoid overhydration to have easier time dealing with acute respiratory syndrome, as less fluid will build up in the lungs.
[Sleep]: 8 hours of sleep is recommended. Again, this is just important overall, and too little sleep will impair immune function and raise your oxidative stress, which is something you don't need.
[Garlic] (Allium sativum L.): a potential unique therapeutic food rich in organosulfur and flavonoid compounds to fight with SARS-2
https://archive.vn/pXV3E
[]
>Mitigation of the replication of SARS-CoV-2 by nitric oxide in vitro
https://archive.vn/TUNPr
>The 10 Best Foods to Boost Nitric Oxide Levels
https://archive.is/KjYgk
>garlic
[]
>Severe SARS-2 Is Fueled by Disrupted Gut Barrier Integrity
>In an intestinal obstruction mouse model, pretreatment with a citrulline-rich diet preserved gut barrier integrity
https://archive.vn/nBcdZ
https://www.medrxiv.org/content/10.1101/2020.11.13.20231209v1.full.pdf
>Foods Containing L-Citrulline
https://archive.vn/eLAd9
>garlic
[]
>Many reports on SARS-2 associated with the amplified incidence of thrombotic events
>Along with that endothelial dysfunction activates the complement system pathways and contributes to the acute and chronic inflammation via cytokine storm with the production of the cytokines and chemokines, coagulation in different organs and further leads to multi-organ failure
https://archive.vn/zDJx2
>Blood-thinning foods, drinks, and supplements
https://archive.vn/1ozU4
>garlic
[]
>SARS-CoV-2 infection pathogenesis is related to oxidative stress as a response to aggression
>we suggest a therapeutic strategy to reduce oxidative stress using antioxidants
https://archive.vn/snipt
>Antioxidants
https://archive.vn/VrkVg
>garlic
[]
Inflammation: the key factor that explains vulnerability to severe SARS-2
Immunomodulation and Anti-Inflammatory
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4417560/
>garlic
[]
Discovery of alliin as a putative inhibitor of the main protease of SARS-CoV-2 by molecular docking
>Alliin is the main active component of garlic
https://archive.vn/pHLe9
[]
Bioactive components from garlic on brain resiliency against neuroinflammation and neurodegeneration
https://www.spandidos-publications.com/10.3892/etm.2019.8389
[]
Supplementation with aged garlic extract improves both NK and γδ-T cell function: A randomized, double-blind, placebo-controlled nutrition intervention
https://archive.vn/Z3rRk
[]
Allicin inhibits SDF-1α-induced T cell interactions with fibronectin and endothelial cells
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1782446
[]
If smelling not good is a bit of a problem, then raw apples, lemons, spinach, lettuce, green tea and chew gum would help a bit
https://www.sciencedaily.com/releases/2016/09/160923083806.htm
[Zinc]: Found in highest concentrations in oysters and beef as well as in other seafoods, meats, and garlic. Extremely important to immune function relating to coronavirus.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7247509
Zinc is tolerable up to 100 mg/day for prophylactic purposes (but perhaps 75 mg/day would be more fitting, and up to 150 mg/day for post-exposure/treatment purposes as well
https://lpi.oregonstate.edu/mic/minerals/zinc
[]
Food rich in zinc
https://healthwholeness.com/nutrition/foods-high-in-zinc
As zinc supplementation depletes copper, mind replenishing your copper levels as well (and moderate amounts of copper are beneficial against SARS-2, yes)
[Copper] - not above 10 mg/day
https://lpi.oregonstate.edu/mic/minerals/copper
https://www.sciencedirect.com/science/article/pii/S0306987720308136
Food rich in copper
https://www.copperh2o.com/blogs/blog/ultimate-guide-to-foods-with-copper
[Green tea] and/or [black tea]
Preferably only tea and not tea extract pills, as the latter have a chance to cause liver injury (https://archive.is/XCEtv https://archive.is/dnaHa)
Teas contain Epigallocatechin-gallate (EGCG) which is a zinc ionophore that helps your cells to absorb zinc that halts viral replication in your cells.
https://archive.4plebs.org/pol/thread/269996302/#269996302
[]
Rapid inactivation in vitro of SARS-CoV-2 in saliva by [black tea] and [green tea]
https://www.biorxiv.org/content/10.1101/2020.12.28.424533v1
[]
Bioactive compounds found in [green, black, and oolong tea] possess remarkable antiviral activities against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
>Significant inactivation of SARS-CoV-2 by a green tea catechin, a catechin-derivative and galloylated theaflavins in vitro
>results strongly suggest that EGCG, and more remarkably TSA and galloylated theaflavins, inactivate the novel coronavirus
https://archive.vn/yZHA6
[]
Antiviral activity of [green tea] and plant juices ([black chokeberry (Aronia melanocarpa) juice], [pomegranate (Punica granatum) juice]) against SARS-CoV-2 and influenza virus in vitro
https://www.biorxiv.org/content/10.1101/2020.10.30.360545v1
[Green tea, muscadine grapes, cacao powder, and dark chocolate - able to bind to a particular enzyme, or protease, in the virus and stop it reproducing]
https://archive.vn/9Xzic
[]
Docking Characterization and in vitro Inhibitory Activity of Flavan-3-ols and Dimeric Proanthocyanidins Against the Main Protease Activity of SARS-Cov-2
>To further substantiate the inhibitory activities, extracts prepared from [green tea (GT), two muscadine grapes (MG), cacao, and dark chocolate (DC)], which are rich in CAG, ECG, GAG, EGCG, or/and PB2, were used for inhibitory assay. The resulting data showed that GT, two MG, cacao, and DC extracts inhibited the Mpro activity with an IC50 value, 2.84 ± 0.25, 29.54 ± 0.41, 29.93 ± 0.83, 153.3 ± 47.3, and 256.39 ± 66.3 μg/ml, respectively. These findings indicate that on the one hand, the structural features of flavan-3-ols are closely associated with the affinity scores; on the other hand, the galloylation and oligomeric types of flavan-3-ols are critical in creating the inhibitory activity against the Mpro activity.
https://archive.vn/g7Izq
[]
[Green tea] Significant inactivation of SARS-CoV-2 by a green tea catechin, a catechin-derivative and galloylated theaflavins in vitro
https://www.biorxiv.org/content/10.1101/2020.12.04.412098v1
[]
[Catechins]
>Catechins as Potential Mediators of Cardiovascular Health
https://www.ahajournals.org/doi/full/10.1161/ATVBAHA.117.309048
[]
Catechin and curcumin interact with S protein of SARS-CoV-2 and ACE2 of human cell membrane: insights from computational studies
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7820253
[]
Sources of catechins
https://archive.vn/e4yJy
https://www.cleaneatingmag.com/clean-diet/food-health-news/10-ways-to-get-your-catechin-fill
[N-Acetylcysteine] (NAC supplements aren't a bad idea, food sources as well (N-acetyl cysteine is the supplement form/derivative of cysteine amino acid))
600 mg/day for prophylaxis, 1,200 mg/day for treatment
>Antioxidant N-acetyl-L-cysteine (NAC) supplementation reduces reactive oxygen species (ROS)-mediated hepatocellular tumor promotion of indole-3-carbinol (I3C) in rats
https://pubmed.ncbi.nlm.nih.gov/22129741
[]
Food sources
https://www.livestrong.com/article/531520-food-sources-of-n-acetyl-cysteine
>400 gram of pork a day is dosage of N-AC for lung disease (1,200+ mg)
https://www.myfooddata.com/articles/high-cystine-foods.php
https://www.webmd.com/vitamins/ai/ingredientmono-1018/n-acetyl-cysteine-nac
[Vitamin D]: High levels of vitamin D have been found to correlate with better survival rates with coronavirus (as well as less inflammation). Sun exposure for 30-60 minutes a day is recommended, or D3 supplements. No real need to exceed way further than 15,000 IU per day (upper limit - beyond which toxicity is reported ~39,000 IU, (https://www.healthline.com/nutrition/how-much-vitamin-d-is-too-much#TOC_TITLE_HDR_4 https://pubmed.ncbi.nlm.nih.gov/28768407), may make sense to consider only if you're not getting direct sunlight exposure (not through glass, but exactly direct)), but reduce dosage if any side effects occur. Citrus juice, butter and/or some vit K supplementation could help preventing possible side-effects (https://pubmed.ncbi.nlm.nih.gov/16482864/)
[]
[Vitamin D]-Inducible Peptide LL-37 Inhibits Binding of SARS-CoV-2 Spike Protein to its Cellular Receptor Angiotensin Converting Enzyme 2 In Vitro
>This study supports the prophylactic use of vitamin D to induce LL-37 that protects from SARS-CoV-2 infection, and the therapeutic administration of vitamin D for the treatment of COVID-19 patients. Further, our results provide evidence that the direct use of LL-37 by inhalation and systemic application may reduce the severity of COVID-19.
https://www.biorxiv.org/content/10.1101/2020.12.02.408153v2
[]
[Vitamin D] deficiency raises SARS-CoV-2 infection risk by 77%, study finds
>Vitamin D deficiency increases a person's risk for catching COVID-19 by 77% compared to those with sufficient levels of the nutrient, a study published Thursday by JAMA Network Open found.
>As many as one in four of the nearly 500 participants in the study were found to have less-than-optimal levels of vitamin D, the data showed.
>Among those found to be lacking the key nutrient, 22% contracted COVID-19, the data showed.
>Of the 60% of study subjects with adequate vitamin D levels, just 12% were infected, according to the researchers.
https://archive.is/GfRhC
[]
Analysis of [vitamin D] level among asymptomatic and critically ill SARS-2 patients and its correlation with inflammatory markers
>The fatality rate was high in vitamin D deficient (21% vs 3.1%). Vitamin D level is markedly low in severe COVID-19 patients. Inflammatory response is high in vitamin D deficient COVID-19 patients. This all translates into increased mortality in vitamin D deficient COVID-19 patients.
>As per the flexible approach in the current COVID-19 pandemic authors recommend mass administration of vitamin D supplements to population at risk for COVID-19
https://archive.vn/VkDQY
[More overly detailed info on vit D and SARS-2]
https://archive.vn/i9VPG
https://archive.vn/oV4ew
[Vitamin B (B3 (aka PP, aka niacin) especially)]
https://pubmed.ncbi.nlm.nih.gov/32707945/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7428453/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7599934/
[]
[Kvas (homemade)] would be useful here, especially with probiotic, antioxidant properties and being rich in nutrients
>Kvass is a soft drink, providing only low energy approximately 32 kcal / 100 g (i.e. approx. 240-320 kcal / l). It is a rich source of B vitamins, including thiamine (B1), niacin (PP), riboflavin (B2) and pyridoxine (B6). There is also a lot of folate, because yeasts - e.g. Saccharomyces cerevisiae, Candida milleri, Torulaspora delbrueckii are able to produce it. This drink has a positive effect on metabolism, and at the same time eliminates flatulence, hyperacidity and other digestive disorders
>as a product of lactic - alcohol fermentation it does not require a pasteurization, and contains mainly lacticc acid bacteria, i.e. useful microflora of the human body. Moreover, kvass contains natural organic acids, sugars and amino acids, which play an important role from the nutritional and physiological point of view. The primary metabolite of lactic acid bacteria, lactic acid, not only increase the bioavailability of calcium and other minerals, but also possesses an antioxidant properties. Products of yeast cells autolysis can enrich kvass environment with a number of valuable components, e.g. superoxide dismutase, able to "scavenge" excess of superoxide radicals (Dziugan, 2008). Kvass as the beverage can be considered a probiotic, but it should be prepared by natural fermentation (not from concentrate) and with no further thermal stabilization
https://www.researchgate.net/publication/275252793_Health_benefits_of_kvass_manufactured_from_rye_wholemeal_bread
[]
Has around ~18 mg of niacin per 100 gram
[Vitamin B12] as well
>Drug repurposing based on a Quantum-Inspired method versus classical fingerprinting uncovers potential antivirals against SARS-CoV-2 including vitamin B12
https://www.biorxiv.org/content/10.1101/2021.06.25.449609v1
[]
Foods rich in vitamin B12
https://www.healthline.com/nutrition/vitamin-b12-foods
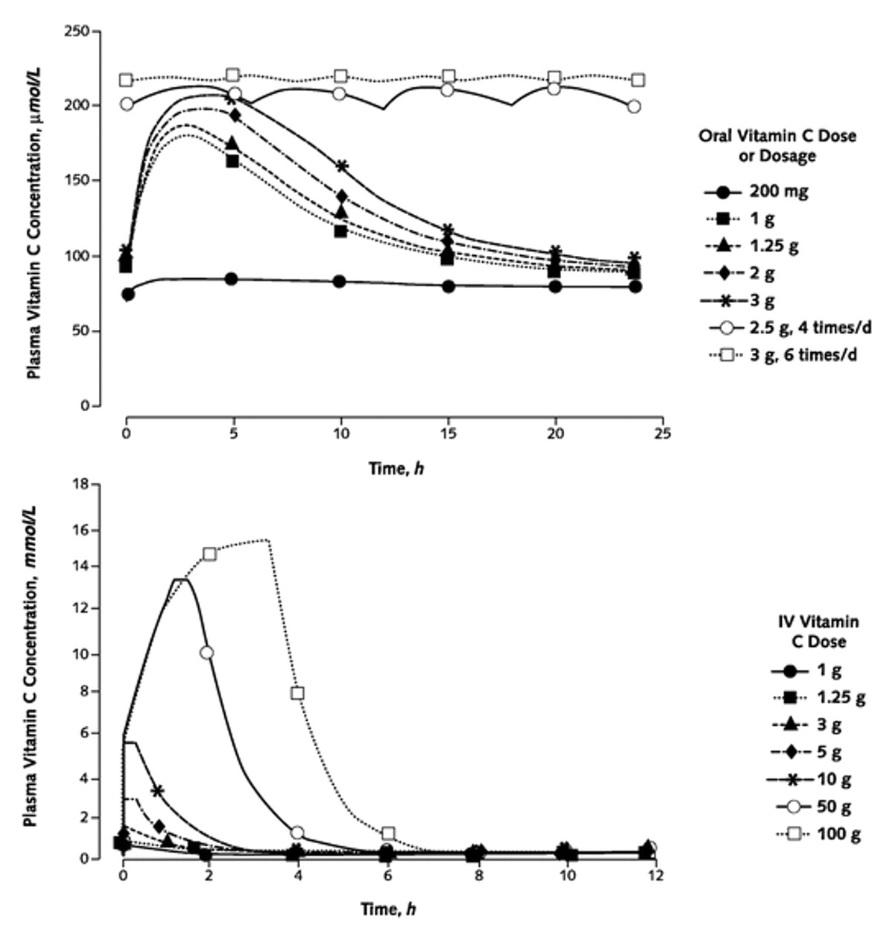
[Vitamin C]: Important for immune function and may be protective in the respiratory tract against coronaviruses. Doses up to 2000 mg are considered relatively safe and without side effects. Good dietary sources are citrus fruit, peppers, and other fruits. Vitamin C is unlikely to be dangerous in doses larger than 2000 mg a day, but may cause diarrhea or possibly kidney stones if sustained for a long period.
You can megadose (don't mistake with overdose) vitamin C by taking ~3g every few hours to keep your concentration levels maxed out.
https://www.thehealthcloud.co.uk/liposomal-vitamin-c-vs-regular-vitamin-c-supplements/
[]
>oral vitamin C (2-8 g/day) may reduce the incidence and duration of respiratory infections and intravenous vitamin C (6-24 g/day) has been shown to reduce mortality, intensive care unit (ICU) and hospital stays, and time on mechanical ventilation for severe respiratory infections
>SARS-2: Up to 82% critically ill patients had low Vitamin C values
https://archive.is/tFtXA
[Nitric oxide oxide or sources of L-arginine] (NO nasal/oral sprays would be quite useful as well) (NO - don't confuse with nitrous oxide N2O)
Mitigation of the replication of SARS-CoV-2 by nitric oxide in vitro
https://archive.vn/TUNPr
[]
What would help with getting nitric oxide
https://www.healthline.com/nutrition/nitric-oxide-foods
https://www.healthline.com/nutrition/nitric-oxide-supplements#TOC_TITLE_HDR_4
[]
Clinical efficacy of nitric oxide nasal spray (NONS) for the treatment of mild SARS-2 infection
>Patients in both trial groups started on NONS or placebo at least 4 days after the onset of symptoms and were well balanced in terms of risk factors (Table 1 ). 34 (85%) of the NONS group and the placebo group were determined to be lineage B.1.1.7 (VOC202012/01) and the remainder were not determined to be a variant of concern. There were no serious adverse events in patients within either trial group. NONS versus placebo started on at least day 4 of symptom onset was independently associated with an accelerated decrease in log(10) SARS-CoV-2 RNA concentration of −1.21 (95% CI, −2.07 to −0.35; P=0.01) and −1.21 (95% CI, −2.19 to −0.24; P=0.02) on days 2 and 4 respectively (Fig. 1 ). Mean SARS-CoV-2 RNA concentration was lower on NONS by a factor of 16.2 at days 2 and 4. A rapid reduction (95%) in the SARS-CoV-2 viral load was observed within 24 hours, with a 99% reduction observed within 72 hours with NONS treatments.
>The mean SARS-CoV-2 RNA concentration at day 6 was lowered to −3.32 on NONS, with a treatment difference of −0.98 (95% CI, −2.04 to 0.08; P=0.069). The mean treatment difference using an area under curve estimate from baseline through day 6 was −5.22 with a 95% CI, −9.14 to −1.31; P=0.001), where the mean change was −10.17 for the NONS group and −4.95 for the placebo group.
>40 subjects (15 NONS and 25 placebo subjects) completed and returned the trial assessment questionnaire. A total of 46.7% (7 of 15) of NONS respondents reported feeling better versus 8% (2 of 25) of placebo respondents on treatment. NONS subjects typically reported being better by day 2-4 on treatment, whereas the placebo subjects typically did not report feeling better until after day 5.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8117664/
[L-serine]
Combined metabolic cofactors supplementation (CMCS) consisting of L-serine, N-acetyl-L cysteine (NAC), nicotinamide riboside (NR, aka nicain, aka vitamin B3), and L-carnitine tartrate is being studied for the treatment of patients with SARS-2 (everything aside L-serine is expanded on in this paste in other sections, CTRL+F the entries' partial names/alternative names)
>We conducted a placebo-controlled, phase-2 clinical trial involving ambulatory COVID19 patients. A total of 100 patients were randomly assigned on a 3:1 basis to HCQ plus CMCS or HCQ plus placebo. The total treatment period for the hydroxychloroquine was 5 days, and for the CMCS/placebo was 14 days. Clinical status was evaluated daily by phone, using a binomial scale for subject reported presence or absence for multiple COVID-19 related symptoms. Plasma samples for clinical chemistry analyses were collected on day 0 and day 14.
>93 patients
>CMCS with hydroxychloroquine significantly reduced the average complete recovery time compared with hydroxychloroquine and placebo (6.6 days vs 9.3 days, respectively). Moreover, there was a significant reduction in ALT, AST and LDH levels on day 14 compared to day 0 in the hydroxychloroquine plus CMCS group. The adverse effects were uncommon and self-limiting.
>CMCS resulted in a significant reduction in recovery time and liver enzymes associated with hepatic function
>CMSC is associated with a low incidence of adverse events
https://www.medrxiv.org/content/10.1101/2020.10.02.20202614v1.full.pdf
[]
Food sources of L-serine
https://bioserine.com/blogs/l-serine-foods/good-sources-of-l-serine-in-foods
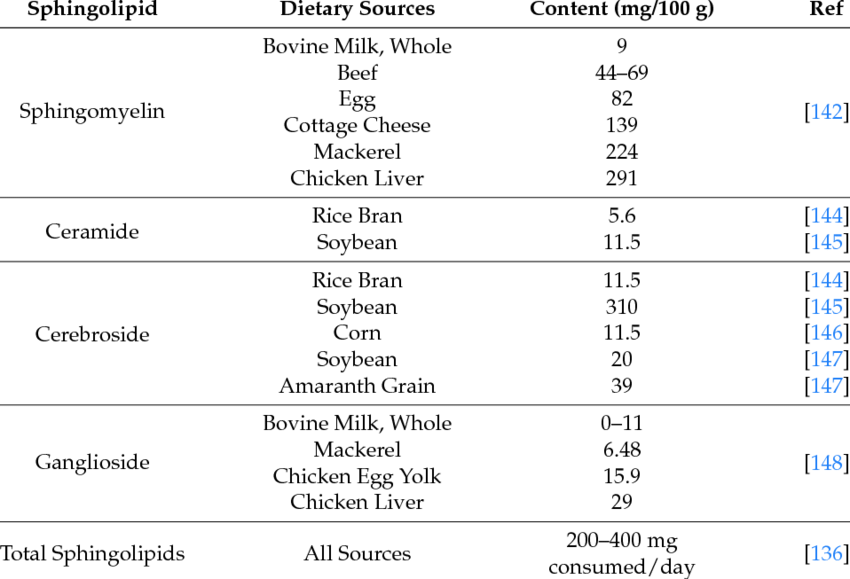
[Sphingolipids]
>Bioactive sphingolipids play a crucial role in the regulation of viral infections and pro-inflammatory responses involved in the severity of SARS-2
[]
Sources of sphingolipids
https://www.researchgate.net/figure/Sphingolipid-content-of-foods_tbl1_320880681
https://academic.oup.com/jn/article/129/7/1239/4722573
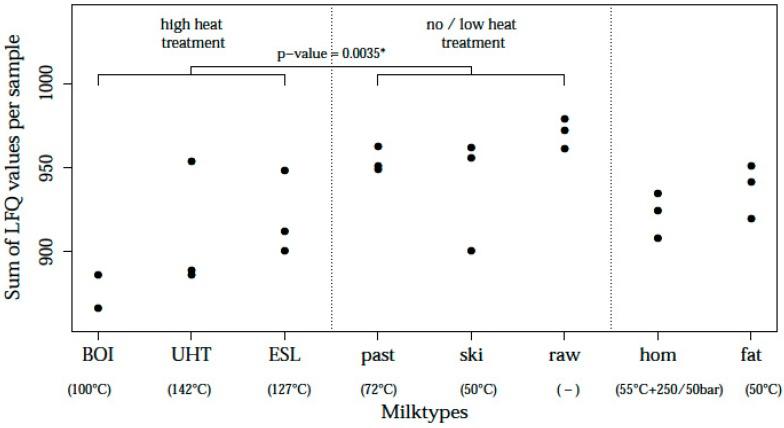
[Lactoferrin]: Binds to co-receptors on the cell wall that coronavirus uses to bring itself in, reducing chance of infection. Also is an anti-inflammatory, anti-oxidant, and an inhibitor of cholesterol accumulation in mitochondria. More of it is found in thermally unprocessed cheeses and milk (raw milk, HTST-pasteurized milk), as well as supplements. Doesn't seem possible to overdose on cheese, supplements may cause runny stool if too much is taken.
>Minimum 100mg for prophylactic purposes
>Minimum 300mg daily for treatment purposes
Non-supplement form is contained in dairy (0.174 g/l in low heat pasteurized cow’s milk (and 1.2 g/kg in semihard cheese produced from that milk))
Maximum dose is ~1.5g and ~3.5g for prophylactic and treatment purposes respectively
[]
Cow’s milk is the most readily available source of lactoferrin, with an average concentration of 0.174 g/l in low heat pasteurized cow’s milk (and 1.2 g/kg in semihard cheese produced from that milk) [129], which is in good agreement with other studies, though the range experienced (0.03–0.486 g/l) is dependent on several factors
https://sci-hub.hkvisa.net/DOI:10.2217/fvl-2020-0170
[]
The acceptable intake level (AIL) of Lactoferrin sourced from dietary supplements ranges from 10 to 1200mg per day
https://lactezin.com/lactoferrin-dosage-just-how-much-is-enough-for-acne
For treating diseases like hepatitis C, a dose of 1.8 to 3.6 grams per day of bovine lactoferrin has been used in research studies
https://www.verywellhealth.com/the-benefits-of-lactoferrin-89471
[]
https://nutraceuticalbusinessreview.com/news/article_page/Lactoferrin_tested_in_the_fight_against_Covid-19/172056
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7664603/
https://www.frontiersin.org/articles/10.3389/fimmu.2020.01221/full
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7271924/
[]
Lactoferrin contents differ between milk preparation
https://pubmed.ncbi.nlm.nih.gov/33248159/
[]
Lactoferrin as potential supplementary nutraceutical agent in SARS-2 patients: in vitro and in vivo preliminary evidences (100mg daily used)
>A total of 92 mild-to-moderate (67/92) and asymptomatic (25/92) COVID-19 patients were recruited and divided in 3 groups according to the administered regimen. Thirty-two patients, 14 hospitalised and 18 in home-based insolation received oral and intranasal liposomal bovine lactoferrin (bLf), 32 hospitalised patients were treated with standard of care treatment (hydroxychloroquine, azitromicin and lopinavir/darunavir), and 28, in home-based isolation, did not take any medication. Furthermore, 32 COVID-19 negative, not-treated, healthy subjects were added as a control group for ancillary analysis.
>bLf-supplemented COVID-19 patients obtained an earlier and significant (p < 0,0001.) median rRT-PCR SARS-COV-2 RNA negative conversion than standard of care-treated and non-treated COVID-19 patients (14.25 vs 27.13 vs 32.61 days, respectively).
>In addition, bLf-supplemented COVID-19 patients showed significant fast clinical symptoms recovery than standard of care-treated and non-treated COVID-19 patients. Moreover, in bLf-supplemented patients, a significant decrease of either serum ferritin or IL-6 levels or host iron overload, all parameters characterizing inflammatory processes, were observed. Serum D-dimers was also found significantly decreased following bLf supplement. No adverse events were reported.
>These in vitro and in vivo observations led us to speculate a potential and safe supplementary role of Blf in the management of mild-to-moderate and asymptomatic COVID-19 patients.
https://www.biorxiv.org/content/10.1101/2020.08.11.244996v4
[]
Lactoferrin decreases LPS-induced mitochondrial dysfunction in cultured cells and in animal endotoxemia model
>lactoferrin protects against oxidative insult at the mitochondrial level
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3030479
[]
Lactoferrin (contained in unprocessed or lownly processed dairy) as an immunomodulator
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2915836
[]
As an inhibitor of cholesterol accumulation in macrophages
https://pubmed.ncbi.nlm.nih.gov/8011684
[Carnitine] supplements or food rich in carnitine
Food sources
https://ods.od.nih.gov/factsheets/Carnitine-HealthProfessional/#h3
[]
Mendelian randomization analyses show that higher acetyl-carnitine and carnitine levels in blood protect against severe SARS-2
>[...] a 40% reduction in risk associated with a doubling of carnitine or acetyl-carnitine (carnitine odds ratio (OR) = 0.56, 95% confidence intervals (CI) 0.33 to 0.95, p=0.03 and acetyl-carnitine OR=0.60, 95% CI 0.35 to 1.02, p=0.06), and evidence of protective effects on hopitalisation with Covid19.
>For acetyl-carnitine the largest protective effect was seen in the comparison between those hospitalised with Covid19 and those infected but not hospitalised (OR=0.34, 95%CI 0.18 to 0.62, p=0.0005)
https://www.medrxiv.org/content/10.1101/2021.05.31.21257910v1
[Anti-oxidants] - from supplements or food, preferably food
SARS-CoV-2 infection pathogenesis is related to oxidative stress as a response to aggression
>we suggest a therapeutic strategy to reduce oxidative stress using antioxidants
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7357498/
[]
Handy list including food sources:
https://naturalhealthtechniques.com/list-of-antioxidants/
[Turmeric] could have antiviral properties
http://archive.is/OCIiB
https://www.frontiersin.org/articles/10.3389/fphar.2021.583387/full
[Curcumin] has high binding affinity towards nucleocapsid and nsp 10 proteins with potential antiviral activity
http://archive.is/mv9WI
[]
Oral Curcumin With Piperine as Adjuvant Therapy for the Treatment of SARS-2: A Randomized Clinical Trial
>Patients with mild, moderate, and severe symptoms who received curcumin/piperine treatment showed early symptomatic recovery (fever, cough, sore throat, and breathlessness), less deterioration, fewer red flag signs, better ability to maintain oxygen saturation above 94% on room air, and better clinical outcomes compared to patients of the control group. Furthermore, curcumin/piperine treatment appeared to reduce the duration of hospitalization in patients with moderate to severe symptoms, and fewer deaths were observed in the curcumin/piperine treatment group.
https://www.frontiersin.org/articles/10.3389/fphar.2021.669362/full
[]
Review/Rundown - Effects of Curcumin on Microglial Cells, usefulness against neuroinflammation and neurodegenerative diseases
>to protect neurons and fight invading pathogens, resting microglia transform to an activated-form, producing inflammatory mediators, such as cytokines, chemokines, iNOS/NO and COX-2
>Excessive inflammation leads to damaged neurons and neurodegenerative diseases (NDs),
>Curcumin is widely used in Asia and has many therapeutic properties, including antioxidant, anti-viral, anti-bacterial, anti-mutagenic, antiamyloidogenic and anti-inflammatory, especially with respect to neuroinflammation and NDs
[...]
https://archive.is/8Op21
[Black pepper] in diet can prevent SARS-2, says IIT(ISM) study
https://archive.vn/3y04k
[]
Black pepper is also a nice antiplatelets, anti‐inflammatory, antioxidant agent and acts on TRP channels involved in the disease
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8217345
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8013177
Foods known to contain [Citrulline] (like garlic) or citrulline dietary supplements (L-citrulline or Citrulline malate)
Sources of citrulline
https://archive.vn/eLAd9
https://www.healthline.com/nutrition/citrulline-supplements
[]
Severe SARS-2 Is Fueled by Disrupted Gut Barrier Integrity
>In an intestinal obstruction mouse model, pretreatment with a citrulline-rich diet preserved gut barrier integrity
https://www.medrxiv.org/content/10.1101/2020.11.13.20231209v1
https://www.medrxiv.org/content/10.1101/2020.11.13.20231209v1.full.pdf
[Peppers] and other foods rich in [capsaicin]
https://www.ga2len.net/PDF/00%20Oral%20capsaicin%20in%20COVID-19.pdf
https://www.mdpi.com/1420-3049/25/24/5888/pdf
https://www.researchgate.net/publication/348203070_Relation_between_Covid-19_and_high_capsaicin_diets
https://www.livestrong.com/article/408453-foods-that-have-capsaicin
Foods rich in [pelargonidin]
>pelargonidin, a natural flavonoid bind and activates the AhR in vitro and reverses intestinal inflammation caused by chronic exposure to high fat diet or to the intestinal braking-barrier agent DSS in a AhR-dependent manner. In these two models, development of colon inflammation associated with upregulation of ACE2 mRNA expression
>Molecular docking studies suggested that pelargonidin binds a fatty acid binding pocket on the receptor binding domain of SARS-CoV2 Spike protein
>In vitro pelargonidin significantly reduces the binding of SARS-CoV2 Spike protein to ACE2 and reduces the SARS-CoV2 replication in a concentration-dependent manner
https://www.biorxiv.org/content/10.1101/2021.02.24.432203v1
[]
>grapes
>ripe raspberries
>strawberries
>blueberries
>blackberries
>cranberries
>saskatoon berries
>chokeberries
>plums
>pomegranates
>red radishes
>kidney beans
https://www.tandfonline.com/doi/abs/10.1300/J492v05n03_10
https://books.google.com.ua/books?id=8JQ4DwAAQBAJ&pg=PA70&redir_esc=y#v=onepage&q&f=false
https://www.sciencedirect.com/science/article/abs/pii/S0308814607008308
https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1755-0238.2010.00107.x
[Melatonin] usage is significantly associated with a 28% reduced likelihood of a positive laboratory test result for SARS-CoV-2 confirmed by reverse transcription–polymerase chain reaction assay.
https://archive.vn/WFGGi
Melatonin attenuates growth factor receptor signaling required for SARS-CoV-2 replication
https://www.melatonin-research.net/index.php/MR/article/view/116
Low melatonin as a contributor to SARS-CoV-2 disease
https://www.melatonin-research.net/index.php/MR/article/view/114
SARS-2: Rational discovery of the therapeutic potential of Melatonin as a SARS-CoV-2 main Protease Inhibitor
https://pubmed.ncbi.nlm.nih.gov/32922174/
https://journals.plos.org/plosbiology/article?id=10.1371/journal.pbio.3000970
https://archive.vn/5MWG7
[]
For prophylaxis measures, recommended dose of melatonin would be 1-10mg per day.
For treatment measures, recommended dose of melatonin would be up to 200mg per day.
[Honey] and [Nigella sativa] aka black caraway, black cumin, nigella, kalojeera, kalonji or kalanji, etc, used as a spice for food or for oils commonly against SARS-2 in Pakistan (HNS-COVID-PK): A multi-center placebo-controlled randomized clinical trial
>Three hundred and thirteen patients - 210 moderate and 103 severe - underwent randomization from April 30 to July 29, 2020.
>Among these, 107 were assigned to HNS whereas 103 to placebo for moderate cases.
>For severe cases, 50 were given HNS and 53 were given placebos. HNS resulted in ∼50% reduction in time taken to alleviate symptoms as compared to placebo (Moderate (4 versus 7 days), Hazard Ratio [HR]: 6.11; 95% Confidence Interval [CI]: 4.23-8.84, P<0.0001 and severe (6 versus 13 days) HR: 4.04; 95% CI, 2.46-6.64, P<0.0001).
>HNS also cleared the virus 4 days earlier than placebo group in moderate (6 versus 10 days, HR: 5.53; 95% CI: 3.76-8.14, P<0.0001) and severe cases (8.5 versus 12 days, HR: 4.32; 95% CI: 2.62-7.13, P<0.0001).
>HNS further led to a better clinical score on day 6 with normal activity resumption in 63.6% versus 10.9% among moderate cases (OR: 0.07; 95% CI: 0.03-0.13, P<0.0001) and hospital discharge in 50% versus 2.8% in severe cases (OR: 0.03; 95% CI: 0.01-0.09, P<0.0001).
>In severe cases, mortality rate was four-fold lower in HNS group than placebo (4% versus 18.87%, OR: 0.18; 95% CI: 0.02-0.92, P=0.029). No HNS-related adverse effects were observed.
>HNS significantly improved symptoms, viral clearance and mortality in COVID-19 patients.
>Thus, HNS represents an affordable over the counter therapy and can either be used alone or in combination with other treatments to achieve potentiating effects against COVID-19.
https://www.medrxiv.org/content/10.1101/2020.10.30.20217364v4.full
>In severe cases, mortality rate was four-fold lower in HNS group than placebo
[]
Don't overdose on honey though
https://doi.org/10.1186/2251-6581-13-23
https://dx.doi.org/10.1111%2Fj.1368-5031.2006.00825.x
https://www.healthline.com/health/diabetes/honey-and-diabetes
[Propolis] ("bee glue")
Efficacy of [propolis] as an adjunct treatment for hospitalized SARS-2 patients: a randomized, controlled clinical trial
>standardized propolis product (EPP-AF) on hospitalized adult COVID-19 patients. Patients received standard care plus propolis at an oral dose of 400mg/day (n=40) or 800mg/day (n=42) for 7 days, or standard care alone (n=42). Standard care included all necessary interventions
>The primary end point was the time to clinical improvement defined as the length of hospital stay or oxygen therapy dependency
>Secondary outcomes included acute kidney injury and need for intensive care or vasoactive drugs.
>Time in the hospital after intervention was significantly shortened in both propolis groups compared to the controls; median 7 days with 400mg/day and 6 days with 800mg/day, versus 12 days for standard care alone.
>Propolis did not significantly affect the need for oxygen supplementation. With the higher dose, significantly fewer patients developed acute kidney injury than in the controls (2 vs 10 of 42 patients)
>Propolis as an adjunct treatment was safe and reduced hospitalization time.
https://www.medrxiv.org/content/10.1101/2021.01.08.20248932v1
[]
Biological activities of propolis are attributed to a variety of chemical constituents such as phenolic acids, phenolic acid esters, flavonoids, terpenoids, artepillin C, caffeic acid, chrysin, galangin, quercetin, apigenin, kaempferol, pinobanksin 5-methyl ether, pinobanksin, pinocembrin, and pinobanksin 3-acetate. Propolis has a wide range of applications because of its pharmacological properties including antioxidant, antimicrobial, antiviral, anti-parasitic, anti-neoplastic, immunomodulatory, anti-inflammatory, and hepatoprotective properties.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7811834
[]
Docking studies were performed for certain components of Egyptian Propolis using Avigan, Hydroxychloroquine and Remdesivir as standard antivirals against both COVID-19 3CL-protease and S1 spike protein
>Docking studies revealed that Rutin and Caffeic acid phenethyl ester showed the highest affinity to both targets. Results showed a significant inhibitory effect of the optimized liposomal formula of Propolis against COVID-3CL protease compared with the Egyptian propolis extract. Interestingly, the inhibition of viral replication of COVID-19 determined by RT_PCR has been significantly enhanced via encapsulation of propolis extract within the liposomal formulation and was comparable to the viral inhibitory effect of the potent antiviral (remdesivir)
https://pubmed.ncbi.nlm.nih.gov/33166584
[Quercetin]: Possesses antiviral activity and many other nice features. Can be gotten in supplement form or found in fruits, citrus fruit, garlic, onions and red onions. Is also a zinc ionophore.
https://www.frontiersin.org/articles/10.3389/fimmu.2020.01451/full
[]
Flavonols and dihydroflavonols inhibit the main protease activity of SARS-CoV-2 and the replication of human coronavirus 229E
>Flavonols and dihydroflavonols are two groups of plant flavonoids.
>In this study, we report docking simulation with two Mpro enzymes and five flavonols and three dihydroflavonols, in vitro inhibition of the SARS-CoV-2 Mpro, and in vitro inhibition of the HCoV 229E replication.
>The docking simulation results predicted that (+)-dihydrokaempferol, (+)-dihydroquercetin, (+)-dihydromyricetin, kaempferol, quercetin, myricentin, isoquercetin, and rutin could bind to at least two subsites (S1, S1', S2, and S4) in the binding pocket and inhibit the activity of SARS-CoV-2 Mpro.
>Their affinity scores ranged from -8.8 to -7.4.
>Likewise, these compounds were predicted to bind and inhibit the HCoV-229E Mpro activity with affinity scores ranging from -7.1 to -7.8.
>In vitro inhibition assays showed that seven available compounds effectively inhibited the SARS-CoV-2 Mpro activity and their IC50 values ranged from 0.125 to 12.9 uM.
>Five compounds inhibited the replication of HCoV-229E in Huh-7 cells. These findings indicate that these antioxidative flavonols and dihydroflavonols are promising candidates for curbing the two viruses.
https://www.biorxiv.org/content/10.1101/2021.07.01.450756v1
[]
>Quercetin could be shown to interact with 3CLpro using biophysical techniques and bind to the active site in molecular simulations. Quercetin, with well-known pharmacokinetic and ADMET properties, can be considered as a good candidate for further optimization and development, or repositioned for COVID-19 therapeutic treatment.
https://pubmed.ncbi.nlm.nih.gov/32745548/
[Taurine, hypotaurine, homotaurine]
>Taurine Supplementation Lowers Blood Pressure and Improves Vascular Function in Prehypertension (Randomized, Double-Blind, Placebo-Controlled Study)
https://sci-hub.hkvisa.net/10.1161/HYPERTENSIONAHA.115.06624
Food sources
https://foodfornet.com/taurine-rich-foods/
https://www.sciencedirect.com/science/article/abs/pii/S0308814621017763
[Quinine] (can be also found in tonic water)
Quinine Inhibits Infection of Human Cell Lines with SARS-CoV-2
>In Vero cells, quinine inhibited SARS-CoV-2 infection more effectively than CQN, and H-CQN and was less toxic. In human Caco-2 colon epithelial cells as well as the lung cell line A549 stably expressing ACE2 and TMPRSS2, quinine also showed antiviral activity. In consistence with Vero cells, quinine was less toxic in A549 as compared to CQN and H-CQN. Finally, we confirmed our findings in Calu-3 lung cells, expressing ACE2 and TMPRSS2 endogenously. In Calu-3, infections with high titers of SARS-CoV-2 were completely blocked by quinine, CQN, and H-CQN in concentrations above 50 µM. The estimated IC50s were ~25 µM in Calu-3, while overall, the inhibitors exhibit IC50 values between ~3.7 to ~50 µM, dependent on the cell line and multiplicity of infection (MOI).
>data indicate that quinine could have the potential of a treatment option for SARS-CoV-2, as the toxicological and pharmacological profile seems more favorable when compared to its progeny drugs H-CQN or CQN
https://www.mdpi.com/1999-4915/13/4/647
[Bromelain] (from pineapples, also available from supplements) improves absorption, may also help inhibit cell entry and inactivate the virus
>Bromelain Inhibits SARS-CoV-2 Infection in VeroE6 Cells
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7523097
>The combination of Bromelain and Acetylcysteine (BromAc) synergistically inactivates SARS-CoV-2
https://www.biorxiv.org/content/10.1101/2020.09.07.286906v2
[Probiotics]
https://draxe.com/nutrition/fermented-foods
Reasons are:
Dysbiosis and structural disruption of the respiratory microbiota in SARS-2 patients with severe and fatal outcomes
https://www.medrxiv.org/content/10.1101/2021.05.19.21257485v1
[]
>Because probiotics can mitigate problems of dysbiosis, inflammation and immune function, and can include direct antimicrobial activities, there may be the potential for a positive contribution against secondary infection co-morbidities in COVID-19. New evidence is emerging that infections secondary to SARS-CoV-2 might contribute to COVID-19 pathology or severity [[46], [47], [48], [49]]. Although an early study suggested relatively little concern across the COVID-19 patient population [50], recent reports are finding increased secondary infections in hospitalized individuals with severe disease, observations that may have some association with immunosuppressive drugs in current treatment regimens
>Outside the COVID-19 context, application of the probiotic strains Lactobacillus rhamnosus GG, Bacillus subtilis and Enterococcus faecalis during clinical trials, showed a significant improvement in patients with ventilator-associated pneumonia, including pathogens of various types, compared with placebo treatment
>In general, probiotic strains themselves, including LAB strains, are well known to be non-pathogenic and non-immunogenic, and therefore are considered safe and not a source of potential secondary infections, themselves
>Along with protective effects reported against influenza A virus, LAB have been reported to promote heterotypic immunity to secondary infections
>Furthermore, probiotics have been reported to provide some protection against biofilm-forming pathogens in the respiratory tract
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7785423
[]
>Lactiplantibacillus plantarum is commonly found in milk products (including kefir), meat and a lot of vegetable fermentations including sauerkraut, pickles, brined olives, Korean kimchi, Nigerian Ogi, sourdough, and other fermented plant material, and also some cheeses, fermented sausages, and stockfish.
>As a probiotic, Pediococcus acidilactici represents a beneficial bacterium often found in dairy products, fermented vegetables, and cured meats as a result of its potent homofermentative properties
[]
[Including cheese]
https://www.researchgate.net/publication/314700426_Cheese_Microbiology_of_Cheese
[]
>INTRANASAL APPLICATION OF LACTOCOCCUS LACTIS W 136 BACTERIA EARLY IN COVID 19 INFECTION MAY HAVE A BENEFICIAL IMMUNOMODULATORY EFFECT: A PROOF-OF-CONCEPT STUDY
>Twenty-three of a planned forty participants aged 18-59 without comorbidities were recruited. Irrigation with intranasal L lactis W136 twice-daily for fourteen days of was associated with a nasal response characterised by increase in the symptom of Facial and Throat pain/discomfort, and with a lesser severity in symptoms of i) Fatigue ii) Olfactory dysfunction and iii) Breathlessness. Safety and tolerability were good, with no acute infections or severe deteriorations. Interpretation: Facial and throat pain may correspond to postulated mechanism of action corresponding to activation of innate defences with antiviral effects and may explain the potentially protective effects seen.
https://www.medrxiv.org/content/10.1101/2021.04.18.21255699v1
[]
Efficacy and safety of novel probiotic formulation in adult SARS-2 outpatients: a randomized, placebo-controlled clinical trial
>Symptomatic Covid 19 outpatients (aged 18 to 60 years) with positive SARS-CoV2 nucleic acids test were randomized to active (n=150; ≥2x109 colony-forming units (CFU) of probiotic strains Lactiplantibacillus plantarum KABP022, KABP023 and KAPB033, plus strain Pediococcus acidilactici KABP021) or placebo (n=150), take orally once daily for 30 days.
>300 subjects were randomized (median age 37.0 years [range 18 to 60], 161 [53.7%] women, 126 [42.0%] having known metabolic risk factors), and 293 completed the study (97.7%).
>Remission was achieved by 78 of 147 (53.1%) in the active group compared to 41 of 146 (28.1%) in placebo (P<0.0001; ARR=25.0%), still significant after multiplicity correction for the primary endpoint. No hospitalizations or deaths occurred during the study, precluding the assessment of efficacy on these endpoints.
>No serious adverse events occurred during the study. Replication studies with this probiotic formula are warranted.
https://www.medrxiv.org/content/10.1101/2021.05.20.21256954v1
A natural food preservative peptide nisin can interact with the SARS-CoV-2 spike protein receptor human ACE2
>Nisin, a food-grade antimicrobial peptide produced by lactic acid bacteria has been examined for its probable interaction with the human ACE2 (hACE2) receptor, the site where spike protein of SARS-CoV-2 binds. Among the eight nisin variants examined, nisin H, nisin Z, nisin U and nisin A showed a significant binding affinity towards hACE2, higher than that of the RBD of the SARS-CoV-2 spike protein
>nisin H acted as a potential competitor of RBD to access the hACE2 receptor
>globally used food preservative, nisin has the potential to bind to hACE2.
https://archive.is/VLguP
[]
>lactic acid bacteria - Lactococcus lactis - used for [cheese] production
>nisin is nice against cancer
>time for designated nisin supplements?
https://archive.is/VLguP
https://archive.is/ntUVz
[Gallic acid], foods rich in it
The vasorelaxant effect of gallic acid involves endothelium-dependent and -independent mechanisms
https://pubmed.ncbi.nlm.nih.gov/26643780/
[]
Gallic acid improves endothelium-dependent vasodilatory response to histamine in the mesenteric vascular bed of diabetic rats
https://pubmed.ncbi.nlm.nih.gov/27943652/
[]
Foods in which the polyphenol Gallic acid is found
http://phenol-explorer.eu/contents/polyphenol/413
[Carrot Pomace Polysaccharide] (CPP) Improves immune response efficacy in Immunosuppressed Mice via Dendritic Cell Activation
>In a mouse model of immunosuppression induced by cyclophosphamide, animals given CPP before and after an influenza vaccine challenge showed increased frequencies of dendritic cells and natural killer cells in the spleen, in addition to the recovery of vaccine-specific antibody titers. Moreover, innate myeloid cells in CPP-fed mice showed evidence of phenotypic modification via markedly enhanced interleukin(IL)-12 and interferon(IFN)-γ production in response to lipopolysaccharide(LPS) stimulation ex vivo
https://pubmed.ncbi.nlm.nih.gov/32916825
[Vitamin A] (retinol/retinolic acid)
Food sources
https://healthfully.com/307889-what-foods-contain-retinoic-acid.html
[]
Retinol Depletion in Severe SARS-2
>Vitamin A is depleted during infections.
>In this study, low retinol levels were found in patients with severe COVID-19.
>Retinoid signaling impairment in COVID-19 disrupts Type-I interferon synthesis.
>patient group consisted of 27 severe SARS-CoV-2 patients hospitalized in the intensive care unit with respiratory failure
>control group consisted of 23 patients without COVID-19 symptoms.
>Retinol levels were found to be significantly lower in the patient group.
>There was no difference in retinol between two different age groups in the patient group. There was no significant difference in retinol between men and women. Comorbidity did not affect serum retinol levels
>Drugs preventing retinol excretion were not stopped in the patient group.
>Some patients took vitamin A externally. Despite this, retinol was low in COVID-19 patients. Retinol depletion impairs Type-I interferon synthesis by impairing retinoid signaling. Retinoid signaling may be the main pathogenetic disorder in COVID-19
>Retinol, retinoic acid derivatives, and some CYP450 inhibitors may work on COVID-19
https://www.medrxiv.org/content/10.1101/2021.01.30.21250844v1
[Vitamin E]: May prevent clotting associated with coronavirus, as well as being associated with vasodilation and reducing inflammation. Recommended daily allowance is ~15mg, can be found in high quantities in oils, peanut butter, and nuts. High doses may interfere with the body's ability to clot blood at wounds, do not exceed ~200mg for a sustained period.
https://www.news-medical.net/news/20210715/Water-soluble-vitamin-E-compounds-directly-inhibit-SARS-CoV-2-replication-and-synergize-with-remdesivir.aspx
[Selenium]
Food sources
https://www.healthline.com/health/selenium-foods
https://blog.publicgoods.com/is-pesto-healthy
[]
Avoid deficiency (as long as you don't overdose somehow)
>Selenium influences the immune response largely through its action in selenoproteins, which function as cellular antioxidants.46 Deficiency appears to enhance virulence or progression of some viral infections47 as evidenced by the relationship between Keshan disease, coxsackievirus B3 and influenza A, which are exacerbated by low Se status. Selenium also has an important role in the modulation of the inflammatory response and cytokine production.48
>Supplementation of selenium improves the immune system response to viruses in deficient individuals.49 Although scarce evidence of this has been demonstrated in humans, limited studies have shown functional outcomes of selenium supplementation on the human immune system. In one trial of UK adults with poor selenium status, supplementation with selenium attenuated poliovirus more rapidly than those given a placebo.50 Caution is advised due to the adverse effects of selenium in high status and it is suggested those who are selenium sufficient should not supplement due to potential adverse effects.
https://nutrition.bmj.com/content/3/1/93
[]
Research hints that lack of Selen deficiency can explain low SARS-CoV-2 deaths in Finland
>The trace element selenium is important for both animals and humans. Selenium is a strong antioxidant, which means, among other things, that it counteracts aging processes, such as calcification of blood vessels. Supply of selenium has a well-documented good preventive effect on cardiovascular disease. Researchers in the USA and England, among others, have written that selenium has a positive effect on our immune system
http://archive.is/j98Je
[Magnesium]: May promote vitamin D functions in protecting the respiratory epithelium and also act to control blood pressure and improve overall health. Can be found in leafy greens, nuts, whole grains, as well as in fortified breakfast cereals. Daily recommended value is ~400mg for men, ~300 for women, if you take supplements they may cause diarrhea if taken in excess. Generally, avoid exceeding 300mg a day in supplements
https://www.news-medical.net/news/20200604/Study-says-vitamin-magnesium-combo-may-reduce-severity-of-COVID-19-in-seniors.aspx
[BONUS NOTES]:
1) Keep your blood iron in standard, optimal range (of 10.74-30.43μmol/l)
What may help:
[Iron chelators]
>curcumin
https://archive.is/b8HVZ
>apocynin, which is derived from the rhizome of Picrorhiza kurroa
>Mucuna pruiens
>garcinia kola
>floranol (a new flavonoid isolated from the roots of Dioclea grandiflora, a vine that grows in Brazil)
>Pycnogenol™ (PYC), a standardized extract composed of a mixture of flavonoids, mainly procyanidins and phenolic acids obtained from a French maritime pine
>Procyanidins extracted from Vitis vinifera
>flavonoids (including quercetin (GARLIC, onion bulbs))
>EGCG (green tea)
>gallic acid
>catechin
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3821171
[]
>food sources of iron
https://www.healthline.com/nutrition/healthy-iron-rich-foods
If you are interested, the reason for this is:
>In multivariate regression analysis only serum iron and ferritin were significantly associated with hospitalization
>doubling of serum iron was associated with a 6.7x lower odd of hospitalization
>Receiver operating characteristic analysis
>An iron concentration<6μmol/l was identified as the best cutoff-point predicting hospitalization. The sensitivity of iron levels at this value was 94.7% with a specificity of 67.9%
https://archive.is/SFnPC
[]
SARS-CoV-2 mimicks hepcidin (via its proteins orf1ab, ORF10, and ORF3a https://archive.fo/JOYH0) and increases ferritin, which leads to release of iron from hemoglobin with transporting it to the cells, causing iron overload, which causes cell death (ferroptosis):
[]
>iron accumulation becomes a vicious cycle. As the levels of iron slowly accumulated in the cell increase for a certain period of time, the cells can continue their functions. At their point, iron levels exceed a threshold, and ferroptosis can result in cell death, which can trigger a viral agent that enters your cell. This process within the cell is a slow process, but when cell death begins from ferroptosis, it begins to provide a huge increase in oxidative stress compounds and immune response in many vital organs
https://archive.vn/uIw5t
[]
which, in result, may lead to multi-organ oxidative stress, which can precipitate the inflammatory/immune over-response (interleukine storm)
There's shit ton of pathology linked to this axis, actually
[]
>Hyperferritinemia may induce a series of direct and indirect (via autoimmunity) injuries to most organs during COVID-19, such as coagulopathies, macrophage activation syndrome, hemochromatosis-like liver injury, and other ferroptosis-driven syndromes
https://archive.is/MowCB
[]
Also, this:
[]
>Low iron mitigates viral survival: insights from evolution, genetics, and pandemics—a review of current hypothesis
https://archive.vn/JCwjx
2) Keep your vitamin K levels not above normal levels, but also prevent deficiency, all in order to avoid blood clots
Vitamin K2: Helpful for improving vitamin D absorption and heart/kidney health, found in cheeses and meats especially, so supplementation may be unnecessary. May cause increased blood clotting, which may worsen the effects of coronavirus, so additional supplements like vitamin pills is discouraged during infection (avoid overdosing, and avoid being deficient)
[]
Foods That Are High in Vitamin K
>daily value (DV) of 120 mcg should prevent insufficiency in most people
https://archive.vn/x6n58
[]
On blood clots
https://archive.vn/nHxsi
https://archive.vn/yqSDA
[]
On deficiency
>low vit K was associated with increased blood levels of desmosine, a biomarker of degradation of elastic fibres in the lungs, suggesting that low vitamin K status could increase the rate of degradation of elastic fibres during severe SARS-2
>authors hypothesised that increased degradation of elastic fibres in the lungs could be due to lack of activated MGP, which is known to protect extracellular matrix proteins such as elastic fibres from calcification and subsequent degradation. MGP is the strongest known inhibitor of tissue calcification in the arterial vessel wall and thus prevents arterial calcification; also highly expressed in the lungs
>Degradation of elastic fibres in the lungs stimulates calcification of elastic fibres. A rising calcium content of the extracellular matrix stimulates the local synthesis of MGP to prevent calcification of the elastic fibres
>MGP synthesised as dp-ucMGP, needs activation by vit K-dependent carboxylation to be able to protect elastic fibres in the extracellular matrix from calcification. These processes could create a, or exacerbate a pre-morbid, vit K deficit during severe disease and increased demand of Vit K
https://www.medrxiv.org/content/10.1101/2020.12.21.20248613v1
3) Try to keep your sugar low!
Elevated blood glucose levels as a primary risk factor for the severity of SARS-2
>We developed machine learning models to mine 240,000 scientific papers openly accessible in the CORD-19 database, and constructed knowledge graphs to synthesize the extracted information and navigate the collective knowledge in an attempt to search for a potential common underlying reason for disease severity. The literature repeatedly pointed to elevated blood glucose as a key facilitator in the progression of COVID-19
>when we retraced the steps of the SARS-CoV-2 infection we found evidence linking elevated glucose to each step of the life-cycle of the virus, progression of the disease, and presentation of symptoms.
>Specifically, elevations of glucose provide ideal conditions for the virus to evade and weaken the first level of the immune defense system in the lungs, gain access to deep alveolar cells, bind to the ACE2 receptor and enter the pulmonary cells, accelerate replication of the virus within cells increasing cell death and inducing an pulmonary inflammatory response, which overwhelms an already weakened innate immune system to trigger an avalanche of systemic infections, inflammation and cell damage, a cytokine storm and thrombotic events.
>We tested the feasibility of the hypothesis by analyzing data across papers, reconstructing atomistically the virus at the surface of the pulmonary airways, and performing quantitative computational modeling of the effects of glucose levels on the infection process.
https://www.medrxiv.org/content/10.1101/2021.04.29.21256294v1
4) Keep your blood calcium levels in the normal range!
>Only patients with serum ionized calcium data from arterial blood gas tests performed at initial evaluation in the ED were included. Ionized calcium levels were expressed both as actually measured levels (AC) and as adjusted mathematically to a standardized pH of 7.4. levels (SC) to avoid influence of sample handling. Hypocalcemia was defined as calcium level below 1.18mmol/L
>We conducted a retrospective cohort study at IRCCS San Raffaele Hospital, a tertiary health-care hospital in Milan, Italy. We included patients (aged≥18 years) with COVID-19 admitted to our Emergency Department (ED). We excluded COVID-19 patients transferred from other hospitals and patients initially hospitalized for other diseases.
>Four hundred twenty-four patients (79.8%) were hospitalized after initial evaluation, they had significantly lower ionized calcium levels as compared to non-hospitalized patients (AC, 1.1 [1.06–1.4] vs 1.14 (1.1–1.18] mmoll/L, p<0.001; SC, 1.13 [1.1–1.17] vs 1.16 [1.12–1.2] mmol/L, p<0.001). In univariate and multivariate analyses, hypocalcemia was an independent risk factor highly associated with hospitalization (AC, p<0.001 SC, p<0.001)
>Thirty-four patients (11.6%) and 33 patients (11.5%), based on AC or SC levels, respectively, developed severe hypocalcemia during hospitalization.
https://archive.is/jtlsm
5) Keep your body pH in normal levels as well!
https://healthfully.com/toxicity-plugin-air-fresheners-6941471.html
https://steptohealth.com/reduce-ph-level-bodies
[]
The long reasoning behind this is:
Lysosomal protein TMEM106B appeared unique to SARS-CoV-2 infection
>SARS-CoV-2 requires the lysosomal protein TMEM106B to infect human cell lines and primary lung cells. TMEM106B overexpression enhanced SARS-CoV-2 infection as well as pseudovirus infection, suggesting a role in viral entry. Furthermore, single-cell RNA-sequencing of airway cells from patients with COVID-19 demonstrated that TMEM106B expression correlates with SARS-CoV-2 infection
https://pubmed.ncbi.nlm.nih.gov/33686287
[]
>inhibition of vacuolar H(+)-ATPases significantly increased the levels of TMEM106B, a finding that may provide an unexpected biochemical link to GRN, because this protein is also strongly increased under the same conditions
https://europepmc.org/article/MED/22511793
(btw vacuolar H(+)-ATPases are also called V-ATPases because "fuck you, get confused" https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1218484)
[]
Proton pump inhibitors do exactly that, inhibit H(+)-ATPases
https://www.drugs.com/drug-class/proton-pump-inhibitors.html
[]
And, interestingly, this adds up with proton pump inhibitor users being more susceptible to SARS-2 infection
https://pubmed.ncbi.nlm.nih.gov/32852340
and more severe SARS-2 disease
https://gut.bmj.com/content/70/1/76
https://europepmc.org/article/PMC/PMC8036156
[]
Since proton pump itself decreases pH via activating H2, M3 and CCK receptors, it would make sense to, you know, just keep your pH in normal values.
Going too low may be a risk in beetus and Parkinsons (especially since Corona-chan can gift you with those), going too high may be a risk in stroke and cancer (Corona-chan would love this!).
[Reminder/recap - diet, exercise]
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3258094
[]
>garlic, cumin, coriander, basil, curcumin (turmeric), cinnamon, black pepper, ginger, cloves (dried/oil), mint, thymol/ajoway, some sloppy mess that consists of honey, ghee, Indian gooseberry and other berries, sesame oil and various herbs
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8082487
[]
Inhibition of PI3K/Akt/mTOR Signaling by Natural Products
>Recent studies have demonstrated that a number of natural products (or nutraceuticals) isolated from plants (e.g. fruits, vegetables, spices, nuts, legumes, herbs, etc.) also inhibit PI3K/Akt/mTOR pathway, and exhibit potent anticancer activities. As most of the natural products occur in our diet every day, and are very safe, the results suggest that those natural products may be explored for cancer prevention and treatment.
>This special issue selects
>apigenin (parsley, celery, lettuce onions, oranges, tea, chamomile, wheat sprouts)
>curcumin
>cryptotanshinone (Salvia miltiorrhiza - red/chinese sage)
>fisetin (fruits and vegetables, such as strawberry, apple, persimmon, grape, onion, and cucumber)
>indoles (cruciferous vegetables such as brussels sprouts, broccoli, bok choy, cabbage and turnips)
>quercetin
>resveratrol (peanuts, pistachios, grapes, red and white wine, blueberries, cranberries, even cocoa, dark chocolate)
>tocotrienol (vegetable oils)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3775843
[]
Diet quality and risk and severity of SARS-2: a prospective cohort study
>data from 592,571 participants of the smartphone-based COVID Symptom Study. Diet quality was assessed using a healthful plant-based diet score, which emphasizes healthy plant foods such as fruits or vegetables.
>Over 3,886,274 person-months of follow-up, 31,815 COVID-19 cases were documented. Compared with individuals in the lowest quartile of the diet score, high diet quality was associated with lower risk of COVID-19 (HR, 0.91; 95% CI, 0.88-0.94) and severe COVID-19 (HR, 0.59; 95% CI, 0.47-0.74). The joint association of low diet quality and increased deprivation on COVID-19 risk was higher than the sum of the risk associated with each factor alone. The corresponding absolute excess rate for lowest vs highest quartile of diet score was 22.5 (95% CI, 18.8-26.3) and 40.8 (95% CI, 31.7-49.8; 10,000 person-months) among persons living in areas with low and high deprivation, respectively.
>A dietary pattern characterized by healthy plant-based foods was associated with lower risk and severity of COVID-19. These association may be particularly evident among individuals living in areas with higher socioeconomic deprivation.
https://www.medrxiv.org/content/10.1101/2021.06.24.21259283v1
[]
Western diet increases SARS-2 disease severity in the Syrian hamster
>Pre-existing comorbidities such as obesity or metabolic diseases can adversely affect the clinical outcome of COVID-19.
>Chronic metabolic disorders are globally on the rise and often a consequence of an unhealthy diet, referred to as a Western Diet. For the first time in the Syrian hamster model, we demonstrate the detrimental impact of a continuous high-fat high-sugar diet on COVID-19 outcome.
>We observed increased weight loss and lung pathology, such as exudate, vasculitis, hemorrhage, fibrin, and edema, delayed viral clearance and functional lung recovery, and prolonged viral shedding.
>This was accompanied by an increased trend of systemic IL-10 and IL-6, as well as a dysregulated serum lipid response dominated by polyunsaturated fatty acid-containing phosphatidylethanolamine, recapitulating cytokine and lipid responses associated with severe human COVID-19.
https://www.biorxiv.org/content/10.1101/2021.06.17.448814v1
[]
Details on diet used:
>Four to six-week-old male Syrian Golden hamsters (ENVIGO) were randomly assigned to either regular rodent chow (Teklad Global 16% Protein Rodent Diet, Envigo) or a HFHS diet for 16 weeks (Purina Chow #5001 with 11.5% Corn Oil, 11.5% Coconut Oil, 0.5% Cholesterol, 0.25% Deoxycholic Acid, and 10% Fructose: Dyets Inc., Dyet#615088).
>[Secondary prophylaxis]
[Exercise] (but ONLY if you're absolutely sure you're not potentially infected and have completely recovered (and cleared the virus), as exercising during disease may have a negative effect on your health and recovery (and lesser gains, if not a negation of the gains if the disease gets bad))
>Muscle Strength Explains the Protective Effect of Physical Activity against SARS-2 Hospitalization among Adults aged 50 Years and Older
https://www.medrxiv.org/content/10.1101/2021.02.25.21252451v1
Irisin (hormone produced during exercise) and SARS-2
>Obesity patients are more susceptible to develop COVID-19 severe outcome due to the role of ACE2 in the viral infection.
>ACE2 is regulated by genes associated with increased (TLR3, HAT1, HDAC2, KDM5B, SIRT1, RAB1A, FURIN and ADAM10) or decreased (TRIB3) virus replication.
>Irisin treatment increased by 3-fold the levels of TRIB3 transcript and decreased the levels of other genes.
>FURIN and ADAM10, associated with increased SARS-CoV-2 replication, are diminished by irisin in human subcutaneous adipocytes.
https://sci-hub.hkvisa.net/doi.org/10.1016/j.mce.2020.110917
Spices to Control SARS-2 Symptoms
>Among the spices with a beneficial effect on human health, [allicin], [capsaicin], [curcumin], [gingerol], [mustard oil], [piperine], and quercetin glucosides are the major ones
https://www.karger.com/Article/FullText/513538#f01
[Nicotine patches] (or other sources of nicotine) (at your risk)
>The relationship between nicotine and ACE2 has been explored in the framework of cardiovascular and lung diseases [27].
>nicotine downregulates the expression and/or activity of ACE2 and AT2R, suggesting a possible contribution of nicotinic acetylcholine receptors (nAChR) in the regulation of ACE2.
>Although a lower incidence of COVID-19 has been described in smokers [30], this possibility has not yet been explored in the framework of viral neuroinfections [30].
>Furthermore, it could be a therapeutic target in SARS-CoV-2 infection.
https://archive.vn/ba7uL
[]
>New (pre-print) study from South Korea finds smokers 67% less likely to be infected with SARS-CoV-2.
https://academic.oup.com/ntr/advance-article/doi/10.1093/ntr/ntab079/6248045?searchresult=1
https://velvetgloveironfist.blogspot.com/2020/06/smoking-and-covid-19-update-plus.html
[]
>Study of a COVID-19 outbreak on a French Navy ship. 76% of crew members got the disease, but smokers were 36% less likely to get it.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7953961/
[]
For sources of nicotine, preferably patches, as
>Microscopic images of human stem cell–derived airway tissue models with cell nuclei (blue) and SARS-CoV-2 virus infected cells (green); tissue exposed to cigarette smoke had 2 to 3 times more infected cells than non-exposed tissue
https://blog.cirm.ca.gov/2020/11/23/cirm-funded-study-shows-how-cigarette-smoke-can-worsen-covid-19-infection-in-the-airways/
[Cinnamon] and [Hop Extracts] as Potential Immunomodulators for Severe SARS-2 Cases
https://www.frontiersin.org/articles/10.3389/fpls.2021.589783/full
[Potassium]: Potassium deficiency has been associated with some cases of coronavirus, and sufficient levels of it are important to overall health. Salmon, bananas, milk, and potatoes are all good sources of it. Daily recommended dose is ~3500mg, with an upper safe limit of ~5000mg depending on intake method
[Etc]
[Cat’s claw (Uncaria tomentosa) stem bark] has antiviral effect against SARS-CoV-2
https://www.biorxiv.org/content/10.1101/2020.11.09.372201v1
[Pomegranate peel] extract shows potential as inhibitor of SARS-CoV-2 virus
https://archive.vn/BtHis
>Unproven/fringe benefits
[Angelica archangelica plant roots and seeds] - first-described recently discovered non-toxic vegetal-derived furocoumarin preclinical efficacy against SARS-CoV-2: a promising antiviral herbal drug
> ICEP4 purified compound (ICEP4) is a recently discovered furocoumarin-related purified compound coming from roots and seeds of Angelica archangelica (herbal drug)
>Successful ICEP4 doses against SARS-CoV-2-challenged cells are within the maximum threshold of toxicity concern (TTC) of furocoumarins as herbal preparation, well-established historical use of ICEP4-related compounds as herbal preparations may point towards an already-safe widely extended remedy, which may be ready-to-go for large-scale clinical trials under EMA emergency regulatory pathway. To the best of authors´ knowledge, ICEP4-related herbal drug can be postulated as a promising therapeutic treatment
https://www.biorxiv.org/content/10.1101/2020.12.04.410340v1
Study reveals potential utility of artemisinin-based treatments against SARS-CoV-2
>in vitro efficacy of extracts from the sweet wormwood plant (Artemisia annua), but also artemisinin, artesunate, and artemether derivatives against the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
>Nonetheless, if we translate these findings to clinical conditions, only artesunate showed EC50 values in the range of clinically achievable plasma and tissue concentrations among the tested extracts and pure compounds.
https://www.news-medical.net/news/20201006/Study-reveals-potential-utility-of-artemisinin-based-treatments-against-SARS-CoV-2.aspx
>related sources
>Water: you need it
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7467030/
>sleep: " "
>Vitamin D
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7276229/
>vitamin C
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7110025/
https://pubmed.ncbi.nlm.nih.gov/9306475/
>Magnesium
https://www.medrxiv.org/content/10.1101/2020.06.01.20112334v2
>Potassium
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2767008
https://efsa.onlinelibrary.wiley.com/doi/full/10.2903/j.efsa.2016.4592
>Vitamin E
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7161532/
>Vitamin K (avoid overdosing, and avoid being deficient)
https://www.preprints.org/manuscript/202004.0457/v1
[Just some fun factoid] Modest effects of dietary supplements during the SARS-2 pandemic: insights from 445 850 users of the COVID-19 Symptom Study app
NOTE: the only result evaluation were rates of testing positive, not infection/disease severity/progression/complications
>In 372 720 UK participants (175 652 supplement users and 197 068 non-users), those taking probiotics, omega-3 fatty acids, multivitamins or vitamin D had a lower risk of SARS-CoV-2 infection by 14% (95% CI (8% to 19%)), 12% (95% CI (8% to 16%)), 13% (95% CI (10% to 16%)) and 9% (95% CI (6% to 12%)), respectively, after adjusting for potential confounders. No effect was observed for those taking vitamin C, zinc or garlic supplements.
Also look at the study limitations
https://nutrition.bmj.com/content/early/2021/04/20/bmjnph-2021-000250
[Exposure-specific prophylaxis and early-to-clearance treatment]
[Nattokinase] (from natto)
Nattokinase offers proteolytic degradation activity of SARS-CoV-2 proteins,
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8276596
[]
would be also useful against amyloid fibrils, associated with SARS-2 or not,
>Nattokinase is capable of degrading amyloid fibrils at neutral pH and normal body temperature, suggesting a role in the treatment of amyloid-related diseases such as Alzheimer disease (AD).52 The ability of NK to dissociate amyloid suggested that NK was a potential drug candidate for amyloid-related disorders and this was confirmed in a recent study involving both in vivo and in vitro models.53 Oral administration of NK in the rat model of AD demonstrated a positive effect in modulation of specific factors in the AD pathway.13 In a rat model of cognitive deficits of AD induced by intoxification of colchicine, nano-nutraceuticals containing NK were demonstrated to enhance the impaired learning and memory capability and to be effective inhibitors in the suppression of amyloid-β and BACE-1 activity, thus suggesting a neuroprotective efficacy of NK.54 Ahmed et al55 demonstrated that NK, at a dose of 360 FU/kg, significantly decreased cholinesterase activity, TGF-β, IL-6, and p53 levels accompanied by a significant increase in Bcl-2 levels as compared with an untreated AD control group. Their data suggested that the neuroprotective effect of NK was due to its proteolytic, anti-inflammatory, and antiapoptotic effects.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6043915/
[]
and clots
>Nattokinase dissolves blood clots by directly hydrolyzing fibrin and plasmin substrate. It converts endogenous prourokinase to urokinase (uPA). It also degrades plasminogen activator inhibitor (PAI-1) and increases the level of tissue plasminogen activator (t-PA).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5372539/
[Oral/nasal sprays]
[Iota-carrageenan spray]
Carragelose is a sulfated polymer from red seaweed and a unique, broadly active anti-viral compound
>In the multicenter, randomized, double-blind, controlled CARR-COV-02 study, 394 healthcare staff were randomly assigned to receive iota-carrageenan nasal spray (N = 199) or placebo (N = 195) four times per day. Both groups had similar gender and age distributions. The percentage of participants that developed COVID-19 was significantly lower in the group that received the iota-carrageenan spray compared to placebo (1.0% vs 5.1%, respectively; relative risk reduction for disease of 80.4 %; 95 % CI = 25-95 % - there is a 95 % chance that the risk reduction is in this range).
>Iota-carrageenan nasal spray was safe and well tolerated
https://www.marinomed.com/en/news/marinomed-biotech-ag-shares-positive-clinical-trial-results-for-iota-carrageenan-nasal-spray-in-the-prevention-of-covid-19-1
https://archive.is/85H0E
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0237480
[Nasal saline spray]
Rapid initiation of nasal saline irrigation to reduce morbidity and mortality in SARS-2 outpatients: a randomized clinical trial compared to a national dataset
>In older outpatients testing positive for SARS-CoV-2 who initiated nasal irrigation rapidly after diagnosis, risk of hospitalization or death was eight times lower than national rates reported by the CDC.
https://www.medrxiv.org/content/10.1101/2021.08.16.21262044v2
[Nitric oxide nasal sprays or supplements]
Clinical efficacy of nitric oxide nasal spray (NONS) for the treatment of mild SARS-2 infection
>Patients in both trial groups started on NONS or placebo at least 4 days after the onset of symptoms and were well balanced in terms of risk factors (Table 1 ). 34 (85%) of the NONS group and the placebo group were determined to be lineage B.1.1.7 (VOC202012/01) and the remainder were not determined to be a variant of concern. There were no serious adverse events in patients within either trial group. NONS versus placebo started on at least day 4 of symptom onset was independently associated with an accelerated decrease in log(10) SARS-CoV-2 RNA concentration of −1.21 (95% CI, −2.07 to −0.35; P=0.01) and −1.21 (95% CI, −2.19 to −0.24; P=0.02) on days 2 and 4 respectively (Fig. 1 ). Mean SARS-CoV-2 RNA concentration was lower on NONS by a factor of 16.2 at days 2 and 4. A rapid reduction (95%) in the SARS-CoV-2 viral load was observed within 24 hours, with a 99% reduction observed within 72 hours with NONS treatments.
>The mean SARS-CoV-2 RNA concentration at day 6 was lowered to −3.32 on NONS, with a treatment difference of −0.98 (95% CI, −2.04 to 0.08; P=0.069). The mean treatment difference using an area under curve estimate from baseline through day 6 was −5.22 with a 95% CI, −9.14 to −1.31; P=0.001), where the mean change was −10.17 for the NONS group and −4.95 for the placebo group.
>40 subjects (15 NONS and 25 placebo subjects) completed and returned the trial assessment questionnaire. A total of 46.7% (7 of 15) of NONS respondents reported feeling better versus 8% (2 of 25) of placebo respondents on treatment. NONS subjects typically reported being better by day 2-4 on treatment, whereas the placebo subjects typically did not report feeling better until after day 5.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8117664/
>[TREATMENTS]
>If infected or suspected to be infected
Continue with your diet and supplements listed above. Perhaps increase the dosage on the potent things, just absolutely do NOT overdose.
Absolutely refrain from working out or straining your heart/body, let your body focus on dealing with the infection. It's a given even if you would be dealing with a flu or a common cold.
Consider [steam inhalation] therapy (found to inactivate SARS-CoV-2 virions)
https://www.news-medical.net/news/20201130/Steam-inhalation-therapy-found-to-inactivate-SARS-CoV-2-virions.aspx
After clearance of the symptoms and the virus, CTRL+F
[After clearance of the symptoms and the virus]
[Melatonin]
Melatonin interferes with SARS-2 at several distinct ROS-related steps
https://www.sciencedirect.com/science/article/pii/S0162013421001938
https://pubmed.ncbi.nlm.nih.gov/32574327
[]
For prophylaxis measures, recommended dose of melatonin would be 1-10mg per day.
For treatment measures, recommended dose of melatonin would be up to 200mg per day.
[>OTC treatments]
Full-dose [blood thinners] decreased need for life support and improved outcomes in hospitalized SARS-2 patients in international trial
https://news.umanitoba.ca/blood-thinners-decreased-need-for-life-support-and-improved-outcomes-in-hospitalized-covid-19-patients/
[Aspirin]: thins blood to prevent blood clots, may inhibit viral replication, and may reduce inflammation at high doses (not overdoses) (Higher doses of aspirin (300mg-900mg) reduce the production of prostaglandins and so relieve pain and inflammation). Should not be taken by anyone under 18 due to risk of Reye's Syndrome
https://archive.vn/zUOdg
[]
Aspirin Use is Associated with Decreased Mortality in Patients with SARS-2: A Systematic Review and Meta-analysis
>We included five retrospective cohort studies which met our inclusion criteria with total of 14065 participants in both groups. There were 6797 participants in the aspirin group and 7268 participants in the non-aspirin group.
>Our results show that the use of aspirin was associated with 53% decrease in mortality compared to non-aspirin in patients with COVID-19 (adjusted HR 0.47, 95% CI 0.35-0.63, P< 0.001, I^2= 47%).
>In the analysis restricted to patients hospitalized for COVID-19, the use of aspirin was associated with a 49% reduction in the risk for in-hospital mortality
https://www.medrxiv.org/content/10.1101/2021.07.08.21260236v1
[]
Association of Mortality and Aspirin Prescription for SARS-2 Patients at the Veterans Health Administration
>Aspirin prescription was discovered to be strongly associated with decreased mortality rates for COVID-19 positive patients enrolled
https://www.medrxiv.org/content/10.1101/2020.12.13.20248147v1
[]
Aspirin Use is Associated with Decreased Mechanical Ventilation, ICU Admission, and In-Hospital Mortality in Hospitalized Patients with SARS-2
https://journals.lww.com/anesthesia-analgesia/Abstract/9000/Aspirin_Use_is_Associated_with_Decreased.95423.aspx
[]
Decreased In-Hospital Mortality Associated with Aspirin Administration in Hospitalized Patients Due to Severe SARS-2
https://europepmc.org/article/med/33913549
[]
>Aspirin use may be associated with improved outcomes in hospitalized COVID-19 patients.
https://pubmed.ncbi.nlm.nih.gov/33093359
[]
Combined Anticoagulant and antiplatelet therapy (aspirin or clopidrogel) is associated with an improved outcome in hospitalized SARS-2 patients: a propensity matched cohort study.
https://www.medrxiv.org/content/10.1101/2021.07.13.21260467v1.full.pdf
[]
American Study Confirms That Aspirin Use Is Associated With Decreased Mortality Risk In SARS-2 Patients
https://www.thailandmedical.news/news/american-study-confirms-that-aspirin-use-is-associated-with-decreased-mortality-risk-in-covid-19-patients
[]
Platelet activation in critically ill COVID-19 patients
>We provide evidence that platelets contribute to COVID-19 severity. Plasma sP-selectin level was associated with severity and in-hospital mortality. Transcriptional analysis identified PPBP/CXCL7 and SELPLG as biomarkers for intubation.
https://archive.is/LwTwP
Soluble P-selectin as a marker of in vivo platelet activation
> Multiple regression analysis showed that the only predictors of sP-selectin levels were platelet number (p<0.001) and collagen-induced lag-phase (p<0.01). Aspirin-treated patients showed a significant reduction of sP-selectin levels by 13% (p=0.021) which significantly correlated with collagen-induced lag-phase (p=0.005).
https://pubmed.ncbi.nlm.nih.gov/18835553
[]
Inflammatory process in Alzheimer's Disease
>in pathological conditions, the presence of COX-1 in the CNS has been linked to inflammation development, whereas COX-2 is associated with neurotoxicity. Microglia surrounding the NPs in AD patient shows a high expression of COX-1, which suggests inflammation
>hCOX-2 overexpression in primary cultures of cortical and hippocampal neurons derived from transgenic mice, accelerates the apoptotic damage induced by Aβ, causing cell cycle abnormalities (Xiang et al., 2002a). COX-2 also promotes amyloid plaque formation in parenchyma and increases prostaglandin E2 production. This increased plaque formation, correlates with an increase in amyloid peptide formation (Aβ 1–40 and Aβ 1–42) through the γ –secretase activation without affecting the APP expression levels (Xiang et al., 2002b). Studies performed in a mouse model using COX-2−/− deficient mice demonstrated that the inflammatory response mediated by Aβ was diminished, which suggested that COX-2 inhibition could be an important target to be use for therapy
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3741576
Aspirin inhibits COX-1 and COX-2
https://www.medicinenet.com/script/main/art.asp?articlekey=164408
[Apixaban], orally available FXa inhibitor anticoagulant, inhibits SARS-CoV-2 replication by targeting its major protease in a non-competitive way
>Blood coagulation factor Xa (FXa) and SARS-CoV-2 major protease (Mpro) share over 80% homology at the three-dimensional protein level
https://www.biorxiv.org/content/10.1101/2021.09.23.461605v1
[]
Coagulation factors directly cleave SARS-CoV-2 spike and enhance viral entry
>factor Xa (FXa) and thrombin can also directly cleave SARS-CoV-2 spike, enhancing viral entry. A drug-repurposing screen identified a subset of protease inhibitors that promiscuously inhibited spike cleavage by both transmembrane serine proteases as well as coagulation factors. The mechanism of the protease inhibitors nafamostat and camostat extend beyond inhibition of TMPRSS2 to coagulation-induced spike cleavage. Anticoagulation is critical in the management of COVID-19, and early intervention could provide collateral benefit by suppressing SARS-CoV-2 viral entry
https://thebiogrid.org/227919/publication/coagulation-factors-directly-cleave-sars-cov-2-spike-and-enhance-viral-entry.html
[]
Apixaban RCT for SARS-2 ICU patients
Ninety percent of patients were non-White, 43% were obese, 90% had acute respiratory distress syndrome, and 76% required mechanical ventilation. Nearly half of (47.6%) also experienced renal dysfunction and required renal replacement therapy. Eighty-six percent of patients received prophylaxis or treatment with UFH or LMWH within the 24-hour period prior to apixaban initiation. Patients were initiated on apixaban for the treatment of suspected or confirmed VTE (67%) or AFib (33%). All coagulation parameters remained abnormal but stable throughout the 10-day monitoring period. No patients experienced any major bleeding events or thrombosis throughout the study period. There were four deaths during the follow-up period, all deemed unrelated to coagulopathy or bleeding.
>Apixaban appeared safe and efficacious in ICU patients with severe COVID-19 disease. These data encourage future trials seeking to optimize anticoagulation strategies in patients with severe COVID-19
https://www.semanticscholar.org/paper/Safety-and-Efficacy-of-Apixaban-For-Therapeutic-in-Wenzler-Engineer/ec7a8b699dda49e43a7b6255a9a5cdd23230930d
[Methylene Blue]
METHYLENE BLUE FOR TREATMENT OF HOSPITALIZED COVID-19 PATIENTS: A RANDOMIZED, CONTROLLED, OPEN-LABEL CLINICAL TRIAL, PHASE 2
>In the MB group, a significant improvement in SpO2 and RR was observed on the 3rd day (for both, p < 0.0001) and also the 5th day (for both, p < 0.0001). In the SOC group, there was no significant improvement in SpO2 (p = 0.24) and RR (p = 0.20) on the 3rd day, although there was a significant improvement of SpO2 (p = 0.002) and RR (p = 0.01) on the 5th day. In the MB group in comparison to the SOC group, the rate ratio of increased SpO2 was 13.5 and 2.1 times on the 3rd and 5th days, respectively. In the MB group compared with the SOC group, the rate ratio of RR improvement was 10.1 and 3.7 times on the 3rd and 5th days, respectively. The hospital stay was significantly shortened in the MB group (p = 0.004), and the mortality was 12.5% and 22.5% in the MB and SOC groups, respectively.
https://www.clinicalandtranslationalinvestigation.com/frame_esp.php?id=375
https://www.biorxiv.org/content/10.1101/2020.08.29.273441v1
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7409924
[Antihistamines (H1, H2)]
https://gut.bmj.com/content/69/9/1592
https://www.medrxiv.org/content/10.1101/2020.05.01.20086694v2
http://archive.is/qPfzI
https://www.researchsquare.com/article/rs-30934/v1
https://pubmed.ncbi.nlm.nih.gov/23572231/
https://archive.4plebs.org/pol/search/text/Ranitidine/country/nl/
[Bismuth subsalicylate (Pepto-bismol)]: May alleviate coronavirus-related diarrhea and possibly help with other symptoms. Do not take with aspirin, as you run the risk of salicylate overdose
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7159583/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7302082/
[Famotidine (Pepcid)]: Associated with reduced risk of death possibly by reducing inflammation by lowering histamine levels. 20-40mg doses are generally well tolerated, though 10mg may be sufficient. Can be taken before infection or symptoms if desired. Take before sleep
https://gut.bmj.com/content/early/2020/06/10/gutjnl-2020-321852
https://www.researchsquare.com/article/rs-30934/v2
[Naxproxen (Aleve)]: An nonsteroidal anti-inflammatory drug, it may also have anti-viral properties
https://clinicaltrials.gov/ct2/show/NCT04325633
https://www.biorxiv.org/content/10.1101/2020.04.30.069922v1.full.pdf
https://www.researchsquare.com/article/rs-21833/v1
[Bromhexine]
>Effect of bromhexine on clinical outcomes and mortality in SARS-2 patients: A randomized clinical trial
>early administration of oral bromhexine reduces the ICU transfer, intubation, and the mortality rate in patients with COVID-19
https://pubmed.ncbi.nlm.nih.gov/32983936
[]
Bromhexine Hydrochloride Prophylaxis of SARS-2 for Medical Personnel: A Randomized Open-Label Study
>The rate of the combined primary endpoint did not differ significantly between the active treatment group (2/25 [8%]) and control group (7/25 [28%]); P = 0.07. A fewer number of participants developed symptomatic infection (confirmed COVID-19) in the treatment group compared to controls (0/25 vs 5/25; P = 0.02).
>Bromhexine hydrochloride prophylaxis was associated with a reduced rate of symptomatic COVID-19. However, the prophylactic treatment was not associated with a lower combined primary endpoint rate, a positive swab PCR test and/or COVID-19
https://www.medrxiv.org/content/10.1101/2021.03.03.21252855v1
[Colchicine] use in patients with SARS-2: a systematic review and meta-analysis
>Six studies, reporting on 5,033 patients, were included in this review. Across the six studies, COVID-19 patients who had colchicine had a lower risk of mortality - HR of 0.25 and OR of 0.36. Among the three observational studies, COVID-19 patients who received colchicine had a lower risk of mortality - HR of 0.25 and OR of 0.21 (95% CI: 0.06, 0.71).
>Among three randomized controlled trials, the summary point estimate suggests a direction toward benefit in mortality that is not statistically significant among patients receiving colchicine versus placebo - OR of 0.49
>Colchicine may reduce the risk of mortality in individuals with COVID-19. Further prospective investigation is warranted to determine the efficacy of colchicine as treatment in COVID-19 patients in various care settings of the disease
https://www.medrxiv.org/content/10.1101/2021.02.02.21250960v3
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(21)00222-8/fulltext
[]
https://rmdopen.bmj.com/content/7/1/e001455
[]
Colchicine VS SARS-2
>The trial opened on April 2, 2020, with randomisation to colchicine starting on March 04, 2021 and stopping on May 26, 2021, because the pre-specified time to recovery futility criterion was met. The primary analysis model included 2755 SARS-CoV-2 positive participants, randomised to colchicine (n=156), usual care (n=1145), and other treatments (n=1454). Time to first self-reported recovery was similar in the colchicine group compared with usual care with an estimated hazard ratio of 0.919 [95% credible interval 0.72 to 1.16] and an estimated increase of 1.14 days [-1.86 to 5.21] in median time to self-reported recovery for colchicine versus usual care. The probability of meaningful benefit in time to recovery was very low at 1.8%. Results were similar in comparisons with concurrent controls. COVID-19 related hospitalisations/deaths were similar in the colchicine group versus usual care, with an estimated odds ratio of 0.76 [0.28 to 1.89] and an estimated difference of -0.4% [-2.7% to 2.4]. One serious adverse event occurred in the colchicine group and one in usual care
https://www.medrxiv.org/content/10.1101/2021.09.20.21263828v1
[]
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4599469/
[Dexamethasone (6mg)]
Dexamethasone 12 mg versus 6 mg for patients with SARS-2 and severe hypoxia: an international, randomized, blinded trial
>Among patients with COVID-19 and severe hypoxia,12 mg did not result in statistically significant more days alive without life support at 28 days than 6 mg. However, the confidence interval around the point estimate should be considered when interpreting the importance of the trial.
https://www.medrxiv.org/content/10.1101/2021.07.22.21260755v1
[Inhaled corticosteroids]
[]
[Inhaled corticosteroids] downregulate SARS-CoV-2-related gene expression in COPD: results from a RCT
>This is the first randomized controlled trial to show that ICS affect the expression of key SARS-CoV-2-related genes in COPD. Their relation to important anti-viral response genes may have critical implications for SARS-CoV-2 susceptibility or COVID-19 severity in this vulnerable population
https://www.medrxiv.org/content/10.1101/2020.08.19.20178368v1
https://www.medrxiv.org/content/10.1101/2020.08.19.20178368v1.full.pdf
[]
Patients with severe SARS-CoV-2 pneumonia treated with glucocorticoids (inhaled corticosteroids are also known as glucocorticosteroids, glucocorticoids, steroids https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4033967) pulses with equivalent doses of prednisone greater than or equal to 250mg have a more favorable evolution (less mortality and less admission to ICU)
>Of the 259 patients enrolled in the study, 67 (25.9%) had an unfavorable evolution, dying or requiring ICU admission>glucocorticoids treatment (any dose) versus no glucocorticoids treatment (OR: 0.71 (0.30-1.66)), treatment with glucocorticoids (≥ 250mg prednisone daily) versus no glucocorticoids treatment (OR: 0.35 (0.11-1.08)) and glucocorticoids treatment (≥ 250mg prednisone daily) versus patients with glucocorticoids doses <250mg prednisone daily or without glucocorticoids treatment (OR: 0.30 (0.10-0.88)).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7867393/
[Nitazoxanide]
>Time to sustained response was not reduced by nitazoxanide (median: 13.28 and 12.35 days for nitazoxanide and placebo). Nitazoxanide treatment provided an 85% reduction in the progression to severe COVID-19 (1/184, [0.5%] nitazoxanide vs. 7/195, [3.6%] placebo). In subjects at high-risk according to CDC criteria, 1/112 (0.9%) of nitazoxanide-treated subjects and 7/126 (5.6%) of placebo-treated subjects experienced progression to severe COVID-19. Treatment led to a 79% reduction in the rate of hospitalization (1/184 [0.5%] nitazoxanide vs. 5/195 [2.6%] placebo). The proportions positive for SARS-CoV-2 RNA and viral load at days 4 and 10 were not reduced. Nitazoxanide was safe and well tolerated.
>Treatment of mild or moderate COVID-19 with a five-day course of oral nitazoxanide was safe and well tolerated and was associated with an 85% reduction in the progression to severe illness.
https://medrxiv.org/content/10.1101/2021.04.19.21255441v1
[]
Impairment of SARS-CoV-2 spike glycoprotein maturation and fusion activity by the broad-spectrum anti-infective drug [nitazoxanide]
nitazoxanide interferes with the SARS-CoV-2 spike biogenesis, hampering its maturation at an endoglycosidase H-sensitive stage, and hindering its fusion activity in human cells. Besides membrane fusion during virus entry, SARS-CoV-2 S-proteins in infected cells can also trigger receptor-dependent formation of syncytia, observed in-vitro and in COVID-19 patients tissues, facilitating viral dissemination between cells and possibly promoting immune evasion. Utilizing two different quantitative cell-cell fusion assays, we show that nitazoxanide is effective in inhibiting syncytia formation mediated by different SARS-CoV-2 spike variants in human lung, liver and intestinal cells
https://www.biorxiv.org/content/10.1101/2021.04.12.439549v1
[]
Efficacy of [Nitazoxanide] in reducing the viral load in SARS-2 patients. Randomized, placebo-controlled, single-blinded, parallel group, pilot study.
>n=46
>13 received placebo
>An interim analysis showed that the ratio of patients with a viral load reduction ≥ 35% from baseline up to day 7 of treatment was significantly greater for Nitazoxanide compared to placebo (47.8% vs. 15.4%; Δ 34.6%; 95% CI: 64.7; 4.6: p = 0.037)
https://www.medrxiv.org/content/10.1101/2021.03.03.21252509v1
[Niclosamide]
https://archive.is/k5b8W
https://www.thelancet.com/journals/lanepe/article/PIIS2666-7762(21)00061-2/fulltext
>The antiparasitic agent, niclosamide,36 extracts from herbal medicines (e.g. glycyrrhizin and baicalin);37 and non-steroidal anti-inflammatory agents such as indomethacin have all been reported to inhibit SARS-CoV in vitro
https://academic.oup.com/jac/article/62/3/437/734735
Niclosamide reverses SARS-CoV-2 control of lipophagy
https://www.biorxiv.org/content/10.1101/2021.07.11.451951v1
[]
>Inhibition of Thrombin Generation by Aspirin Is Blunted in Hypercholesterolemia
https://www.ahajournals.org/doi/10.1161/01.ATV.16.8.948
[Fenofibrate]
The hyperlipidaemic drug fenofibrate significantly reduces infection by SARS-CoV-2 in cell culture models
>To identify drugs to repurpose to treat SARS-CoV-2 infections, we established a screen to measure dimerization of ACE2, the primary receptor for the virus. This screen identified fenofibric acid, the active metabolite of fenofibrate. Fenofibric acid also destabilized the receptor binding domain (RBD) of the viral spike protein and inhibited RBD binding to ACE2 in ELISA and whole cell binding assays. Fenofibrate and fenofibric acid were tested by two independent laboratories measuring infection of cultured Vero cells using two different SARS-CoV-2 isolates. In both settings at drug concentrations which are clinically achievable, fenofibrate and fenofibric acid reduced viral infection by up to 70%. Together with its extensive history of clinical use and its relatively good safety profile, these studies identify fenofibrate as a potential therapeutic agent requiring urgent clinical evaluation to treat SARS-CoV-2 infection.
https://www.biorxiv.org/content/10.1101/2021.01.10.426114v2
[]
>Inhibition of Thrombin Generation by Aspirin Is Blunted in Hypercholesterolemia
https://www.ahajournals.org/doi/10.1161/01.ATV.16.8.948
[Ambroxol]
Ambroxol Hydrochloride Inhibits the Interaction between Severe Acute Respiratory Syndrome Coronavirus 2 Spike Protein’s Receptor Binding Domain and Recombinant Human ACE2
https://www.biorxiv.org/content/10.1101/2020.09.13.295691v1
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7546948
[>Unproven/fringe treatments]
[D-galactose supplements]
>galactosylated glycans on circulating antibodies link Dectin-1 on phagocytes to FcγRIIB on myeloid cells to prevent the inflammation mediated by complement activation. Loss of galactose, as observed during COVID-19, decreases the opportunity to activate this important activation checkpoint, thereby promoting inflammation
https://www.medrxiv.org/content/10.1101/2020.11.13.20231209v1
https://www.medrxiv.org/content/10.1101/2020.11.13.20231209v1.full.pdf
[Larazotide acetate]
>Severe SARS-2 Is Fueled by Disrupted Gut Barrier Integrity
>Zonulin is the only known physiological mediator of tight junction permeability in the digestive tract, where higher levels of zonulin drive increases in tight junction permeability.
>hospitalized individuals with higher plasma levels of zonulin were more likely to die compared to those with lower levels of zonulin
>Preventing zonulin-mediated increase in intestinal permeability by a zonulin receptor antagonist AT1001 (larazotide acetate) decreased the severity and incidence of several inflammation-associated diseases in pre-clinical and clinical studies.
>The strikingly high level of serum zonulin we observed during severe COVID-19, which were associated with inflammation and mortality, raise the question of whether modulators of tight junction permeability (AT-1001) can lessen COVID-19 severity
https://www.medrxiv.org/content/10.1101/2020.11.13.20231209v1
https://www.medrxiv.org/content/10.1101/2020.11.13.20231209v1.full.pdf
>Prescription treatments
[Pricey as fuck]
[Sofosbuvir] protects human brain organoids against SARS-CoV-2
>To determine whether SARS-CoV-2 could target the human brain, we infected iPSC-derived human brain organoids. Our findings show that SARS-CoV-2 was able to infect and kill neural cells, including cortical neurons. This phenotype was accompanied by impaired synaptogenesis. Finally, Sofosbuvir, an FDA-approved antiviral drug, was able to rescue these alterations. Given that there are currently no vaccine or antiviral treatments available, urgent therapies are needed. Our findings put Sofosbuvir forward as a potential treatment to alleviate COVID-19-related neurological symptoms
https://www.biorxiv.org/content/10.1101/2020.05.30.125856v1
[ADDITIONAL COMPILATIONS]
[Natural Killer cell enhancement]
>Supplementation with aged garlic extract improves both NK and gd-T cell function and reduces the severity of cold and flu symptoms: A randomized, double-blind, placebo-controlled nutrition intervention
https://sci-hub.hkvisa.net/10.1016/j.clnu.2011.11.019
[]
Also reservatol
https://archive.is/qDYRS
[]
Also, other flavonoids
https://www.sciencedirect.com/science/article/pii/S0955286316308269
[]
Also zinc
https://pubmed.ncbi.nlm.nih.gov/17150331/
[]
Also rice bran and likely whole grains
Arabinoxylan rice bran (MGN-3/Biobran) enhances natural killer cell-mediated cytotoxicity against neuroblastoma in vitro and in vivo
>MGN-3/Biobran stimulation of NK cells induced a higher expression of the activation-associated receptors CD25 and CD69 than in unstimulated cells
https://pubmed.ncbi.nlm.nih.gov/25541298/
[]
Also sea cucumbers
https://www.sciencedirect.com/science/article/abs/pii/S0141813017326843
[]
Also mushrooms (like turkey tail) (gotta get them polysaccharopeptides and polysaccharides K)
https://pubmed.ncbi.nlm.nih.gov/17506950
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3206987
https://pubmed.ncbi.nlm.nih.gov/15465338
[]
Also vit C
https://pubmed.ncbi.nlm.nih.gov/26898166/
[Interfering with TMPRSS2 binding]
SARS-CoV-2 employ TMPRSS2 for S protein priming for entry
>potential way to reduce the initial site of SARS-CoV-2 infection may be to inhibit the activity of TMPRSS2
>six molecules (Neohesperidin, Myricitrin, Quercitrin, Naringin, Icariin, and Ambroxol) were found to be promising against the TMPRSS2. Binding interactions analysis revealed a number of significant binding interactions with binding site amino residues of TMPRSS2.
https://pubmed.ncbi.nlm.nih.gov/32741259
[]
>Neohesperidin is a flavanone glycoside found in citrus fruits
>derivative of hesperetin
http://www.superfoods-scientific-research.com/natural-remedies/hesperidin-benefits.html
[]
>Myricitrin
https://myintakepro.com/blog/myricetin-in-foods/
https://public.tableau.com/views/MyricetinRichFoods/Dashboard1?:showVizHome=no
[]
>Quercetin
https://www.superfoodly.com/quercetin-foods/
[]
>Naringenin and its glycoside has been found in a variety of herbs and fruits, including
>grapefruit https://pubmed.ncbi.nlm.nih.gov/10812937
>bergamot https://pubmed.ncbi.nlm.nih.gov/17960080
>sour orange https://pubmed.ncbi.nlm.nih.gov/12900888
>tart cherries https://pubmed.ncbi.nlm.nih.gov/10552377
>tomatoes https://pubmed.ncbi.nlm.nih.gov/12652057 https://pubmed.ncbi.nlm.nih.gov/22957841
>cocoa https://www.worldcat.org/issn/1076-5174
>Greek oregano https://pubmed.ncbi.nlm.nih.gov/14616013
>water mint https://pubmed.ncbi.nlm.nih.gov/18372132
>as well as in beans https://pubmed.ncbi.nlm.nih.gov/1421508
[]
>Icariin is the main active compound of the Epimedium plant species
https://selfhacked.com/blog/icariin/
[]
>Ambroxol is one of the synthetic derivatives of vasicine, the active substance in the plant Adhatoda Vasica
https://www.sciencedirect.com/topics/pharmacology-toxicology-and-pharmaceutical-science/ambroxol
[Cathepsin L inhibitors]
An Orally Available Cathepsin L Inhibitor Protects Lungs Against SARS-CoV-2-Induced Diffuse Alveolar Damage in African Green Monkeys
https://www.biorxiv.org/content/10.1101/2021.07.20.453127v1
[]
Cathepsin L in SARS-2: From Pharmacological Evidences to Genetics
https://www.frontiersin.org/articles/10.3389/fcimb.2020.589505/full
[]
Food sources
[Rice]
>several cathepsin inhibitory molecules have been identified in plant and animal foods. Oryzacystatin-I in rice is known to inhibit cathepsin L, but also cathepsin B and cathepsin H
[Corn]
>Corn cystatin-I as well inhibits cathepsin L and cathepsin H
[Pineapple stem]
>bromelain inhibitor VI which is a peptide present in pineapple stem selectively inhibits cathepsin L and at a lesser extent trypsin
[Mammalian milk]
>Mammalian milk has significant contents of cysteine protease inhibitors, such as lactoferrin, β-casein and β-lactoglobulin. The inhibitory effect of β-lactoglobulin B, also at a lower extent that of β-lactoglobulin A, on cathepsins K and L have been observed
https://d197for5662m48.cloudfront.net/documents/publicationstatus/43165/preprint_pdf/106cea004ddeb066b28bf1ce0526c89a.pdf
[Blood-brain barrier (BBB) and blood-testis barrier (BTB) strengthening and maintenance]
[BBB]
Curcumin
https://www.sciencedirect.com/science/article/abs/pii/S1756464615000535
[]
Sulforaphane (broccoli, kale, etc)
https://www.semanticscholar.org/paper/Sulforaphane-improves-cognitive-function-following-Dash-Zhao/249bc30434c942f103e9da7291ef53e9d4cfbdf9
[]
Resveratrol (grapes, red wine, raspberries, dark chocolate, etc)
https://pubmed.ncbi.nlm.nih.gov/27535376/
[]
Melatonin
https://pubmed.ncbi.nlm.nih.gov/31811815
[BTB]
Get your vitamins and try to limit exposure to pollutants:
Influence of PM2.5 on spermatogenesis dysfunction via the reactive-oxygen-species-mediated Mitogenactivated-protein-kinase signaling pathway
>combined therapeutic administration of vitamins C and E can maintain the BTB integrity, reduce oxidative stress and cell apoptosis, and prevent toxic effects
https://medcraveonline.com/JLPRR/JLPRR-06-00212.pdf
[]
Testosterone and cytokines regulate BTB integrity via differential effects on the equilibrium between the kinetics of protein endocytosis and recycling by determining the fate of endocytosed proteins
>androgen was shown to facilitate the trafficking of integral membrane proteins between the cell surface and cytosol, as well as their recycling from the cytosol back to the cell surface instead of enhancing the expression of BTB proteins, which would reinforce barrier integrity
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2804916
[]
>Effect of vitamin D supplementation on testosterone levels in men
https://pubmed.ncbi.nlm.nih.gov/21154195/
[]
>1,25-dihydroxyvitamin D influences a large number of biologic pathways which may help explain association studies relating vitamin D deficiency and living at higher latitudes with increased risk for many chronic diseases including autoimmune diseases, some cancers, cardiovascular disease, infectious disease, schizophrenia and type 2 diabetes
>A three-part strategy of increasing food fortification programs with vitamin D, sensible sun exposure recommendations and encouraging ingestion of a vitamin D supplement when needed should be implemented to prevent global vitamin D deficiency and its negative health consequences.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3897598/
"Maintain your T. Get your sunlight. Eat your fucking eggs."
- Anonymous
[Both]
Avoid chronic sleep loss
https://onlinelibrary.wiley.com/doi/full/10.1111/jsr.12907
Avoid diets overly high in cholesterol
>Cholesterol-enriched diet disrupts the blood-testis barrier in rabbits
>cholesterol-enriched diet increased dramatically and time-dependently lipid deposition in the seminiferous tubules and disrupted the BTB as evidenced by increased IgG staining within the seminiferous tubules. Total protein levels of the tight junction proteins ZO-1 and occludin were increased in the seminiferous tubules of rabbits fed the cholesterol38 enriched diet and the distribution patterns of tight junction proteins were markedly affected including an increased accumulation of tight junction proteins in endosomes.
>Disruption of the integrity of the BTB due to increased plasma levels of cholesterol might play a role in male infertility.
https://sci-hub.hkvisa.net/10.1152/ajpendo.00416.2014
[]
>although the blood brain barrier is usually impermeable to cholesterol, it’s integrity is compromised in the cholesterol-fed rabbit
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3066467
[]
>High Cholesterol Diet Exacerbates Blood-Brain Barrier Disruption in LDLr-/- Mice: Impact on Cognitive Function
>A tenfold elevation in plasma cholesterol levels of LDLr-/-mice was observed after a hypercholesterolemic diet, while in wild-type mice, the hypercholesterolemic diet exposure increased plasma cholesterol levels only moderately and did not induce cognitive impairment. LDLr-/-mice presented memory impairment regardless of the diet. We observed BBB disruption as an increased permeability to sodium fluorescein in the prefrontal cortices and hippocampi and a decrease on hippocampal claudin-5 and occludin mRNA levels in both wild-type and LDLr-/-mice treated with a hypercholesterolemic diet. The LDLr-/-mice fed with a regular diet already presented BBB dysfunction. The BBB-increased leakage in the hippocampi of LDLr-/-mice was related to high microvessel content and intense astrogliosis, which did not occur in the control mice.
>Therefore, LDLr-/-mice seem to be more susceptible to cognitive impairments and BBB damage induced by exposure to a high cholesterol diet. Finally, BBB disruption appears to be a relevant event in hypercholesterolemia-induced brain alterations.
https://pubmed.ncbi.nlm.nih.gov/32925052
[After clearance of the symptoms and the virus]
If you lost your sense of smell (anosmia) or got it distorted (parosmia) and you are interested in getting it back, consider trying "[smell training]"
https://archive.vn/oj4gw
[]
Maybe consider getting a sensory training kit for hop aromas (one anon recommended Yakima's hops).
Something fairly smelly and distinct, with labels so you can determine accuracy.
You could probably jury-rig one at home yourself, with stuff like coffee grounds, cinnamon and so on.
To add, improving your neuroplasticity would help, as much as it would help with negating/reverting any other neuronal damage at least to some degree.
>Data analysis revealed that olfactory training induced alterations in functional connectivity networks. Thus, olfactory training is capable of inducing neural reorganization processes. Furthermore, these findings provide evidence for the underlying neural mechanisms of olfactory training.
https://www.researchgate.net/publication/267737543_Recovery_of_Olfactory_Function_Induces_Neuroplasticity_Effects_in_Patients_with_Smell_Loss
CTRL+F [Stimulation of neuronal growth/plasticity]
CTRL+F [Dealing with possible persistent mast cell activation]
A week or two after you recover, try [intermittent fasting] like specified in the link, as it could potentially help against post-SARS-2 lymphophenia.
https://www.sciencedaily.com/releases/2014/06/140605141507.htm
[]
Fasting also may help with misfolded protein diseases, although the presented evidence is only on cellular level for now
https://www.sciencedaily.com/releases/2021/09/210913135810.htm
https://www.pnas.org/content/118/36/e2101410118
[Stimulation of neuronal growth/plasticity]
>diet (all in the paste, as usual)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2805706/#S5title
[]
>flavonoids
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3575938
[]
>magnesium
https://www.sciencedirect.com/science/article/pii/S0896627309010447
[]
>exercise
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5554572
[]
>sleep
https://archive.is/2GWvk
[Dealing with possible persistent mast cell activation]
Mast cell stabilization
>Mast cell stabilisers and mediator blockers, such as antihistamines and anti-leukotrienes, are widely used in allergic conditions and mast cell disorders, which may have similar respiratory symptoms, and are therefore logical substances to consider in the fight against SARS-CoV-2. (2)
>Mast cell stabilisers include Vitamin D (3), ketotifen (also an antihistamine), sodium cromoglycate, quercetin, luteolin. Vitamin C also has a role in mast cell stabilisation.
https://www.bmj.com/content/370/bmj.m2722/rr-3
[Anti-amyloid / misfolded protein disease / prion section]
[Lichen]
We found that three of the extracts, from Parmelia sulcata, Cladonia rangiferina and Lobaria pulmonaria, were able to reduce prion protein levels below the limit of immunblotting detection, indicating at least two logs of reduction.
>We have found that certain lichens, common, ubiquitous, symbiotic organisms, possess a serine protease capable of degrading prion protein (PrP) from prion-infected animals. The protease functions against a range of prion strains from various hosts and reduces levels of abnormal PrP by at least two logs. We have now tested more than twenty lichen species from several geographical locations and from various taxa and found that approximately half of these species degrade PrP. Critical next steps include examining the effect of lichens on prion infectivity and cloning the protease responsible for PrP degradation. The impact of lichens on prions in the environment remains unknown. We speculate that lichens could have the potential to degrade prions when they are shed from infected animals onto lichens or into environments where lichens are abundant. In addition, lichens are frequently consumed by cervids and many other animals and the effect of dietary lichens on prion disease transmission should also be considered.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3338958/
[]
Cladonia rangiferina — reindeer lichen (primarily in areas of alpine tundra)
https://en.wikipedia.org/wiki/Edible_lichen
https://www.researchgate.net/publication/267029781_Cladonia_lichens_and_their_major_metabolites_as_possible_natural_antioxidant_antimicrobial_and_anticancer_agents
[]
Parmelia sulcata
https://pubmed.ncbi.nlm.nih.gov/22231561
[]
Lobaria pulmonaria
https://www.researchgate.net/publication/259081877_Antioxidant_phenolics_from_Lobaria_pulmonaria_L_Hoffm_And_Usnea_longissima_Ach_Lichen_species
[]
Autophagy induced by resveratrol prevents human prion protein-mediated neurotoxicity
>Resveratrol initiates neuroprotective effects via the activation of autophagy, which protects organelles, cells, and organisms against misfolded protein-disorders
>Resveratrol prevented PrP(106-126)-induced neuronal cell death by activating autophagy. Moreover, resveratrol-induced autophagy prevented the PrP(106-126)-induced reduction in mitochondrial potential and translocation of Bax to the mitochondria and cytochrome c release.
>Our results indicate that treatment with resveratrol appears to protect against neurotoxicity caused by prion protein peptides and the neuroprotection is induced by resveratrol-mediated autophagy signals.
https://pubmed.ncbi.nlm.nih.gov/22465415
[]
Melatonin-induced autophagy protects against human prion protein-mediated neurotoxicity
>Melatonin rescued neuronal cells from PrP(106-126)-induced neurotoxicity by prevention of mitochondrial dysfunction.
>protective effect of melatonin against mitochondrial dysfunction was related with autophagy activation. Melatonin-treated cells were dose-dependently increased in LC3-II, an autophagy marker. Melatonin-induced autophagy prevented a PrP(106-126)-induced reduction in mitochondrial potential and translocation of Bax to the mitochondria and cytochrome c release.
>The results of this study suggest that regulation of melatonin is a therapeutic strategy for prion peptide-induced apoptosis.
https://pubmed.ncbi.nlm.nih.gov/22335252
[]
Lactoferrin protects against prion protein-induced cell death in neuronal cells by preventing mitochondrial dysfunction
>Prion disorder-related neurodegenerative diseases are characterized by the accumulation of prion protein (PrP) scrapie isoform (PrPsc) within the central nervous system. PrPsc induces neuronal cell death by increasing intracellular generation of reactive oxygen species (ROS). Lactoferrin (LF) is an 80 kDa protein, which has antioxidant abilities due to the scavenging of ROS. The effects of LF treatment on PrP (106-126)-mediated neurotoxicity and ROS generation were the focus of this study. LF treatment protected against PrP (106-126)-induced neuronal cell death and decreased ROS generation. The reduced ROS generation prevented PrP (106-126)-induced mitochondrial dysfunction. Moreover, PrP (106-126)-induced protein activation including c-Jun N-terminal kinase and caspase-3 were blocked by LF treatment. These results demonstrated that LF protects neuronal cells against PrP (106-126)-mediated neurotoxicity through the scavenging of ROS and provide evidence that LF treatment prevents neuronal cell death caused by PrP
https://www.spandidos-publications.com/10.3892/ijmm.2012.1198
[]
Homotaurine in mild-to-moderate Alzheimer’s disease – a randomized, double-blind, placebo-controlled, multi-centre study
>The primary planned analyses did not show a significant treatment effect, but were confounded by unexplained variance. Post-hoc analyses showed a significant treatment-related reduction in HV loss. However, there was only a trend towards slowing of decline on the ADAS-cog and no slowing of decline on the CDR-SB. These results must be interpreted in consideration of the limitations of clinical and disease-modification outcome measures and their relationship, the heterogeneity of the disease and the impact of confounding demographic and clinical variables.
https://europepmc.org/article/PMC/3258678
[Mitigate and reverse demyelination]
>Demyelinating lesions after viral infection can be caused by cross-reaction between immune response and host cell components, as well as by lymphocyte and macrophage reaction and lymphokine-mediated damage, and immune cell protease release. The pro-inflammatory state in COVID-19 is associated with increased cytokines ("cytokine storm") that may activate glial cells, leading to demyelination. Additionally, viral infection can trigger the production of antibodies targeted against glial cells
https://www.sciencedirect.com/science/article/pii/S0925443916300163
https://www.livestrong.com/article/500681-foods-that-improve-myelination
https://www.medicalnewstoday.com/articles/315227
[]
High-salt diet suppresses autoimmune demyelination by regulating the blood–brain barrier permeability
>there is no evidence that dietary salt promotes or worsens a spontaneous autoimmune disease. Here we show that HSD suppresses autoimmune disease development in a mouse model of spontaneous CNS autoimmunity.
>We found that HSD consumption increased the circulating serum levels of the glucocorticoid hormone corticosterone. Corticosterone enhanced the expression of tight junction molecules on the brain endothelial cells and promoted the tightening of the blood–brain barrier (BBB) thereby controlling the entry of inflammatory T cells into the CNS.
https://www.pnas.org/content/pnas/118/12/e2025944118.full.pdf
[]
>Sphingolipids are not only structural molecules but also bioactive molecules involved in the regulation of cellular events such as development of the nervous system, myelination and maintenance of myelin stability
https://onlinelibrary.wiley.com/doi/10.1111/jnc.15133
Food sources of sphingolipids
https://www.researchgate.net/figure/Sphingolipid-content-of-foods_tbl1_320880681
https://academic.oup.com/jn/article/129/7/1239/4722573
[Pre-vaccination measures]
Ask for your vaccinator for aspiration before injection, as accidental intravessel injection may make the chances and severity of posisble adverse events even higher.
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciab707/6353927
Megadose on prophylaxis (as mentioned in the introductory tl;dr - for proper basic prophylactic measures, you will need anti-inflammatories and immunomodulators, anti-oxidants, anticoagulants, as well as proper nutrition, plenty of vitamins (keep vitamin K not above average levels though), and average iron and calcium levels in the blood). Don't half-ass it - thanks to surfactants, lipid nanoparticles and adjuvants, most of vaccine types could initially present themselves to be more severe in inflammation and clotting than SARS-2 on average can be.
Notably:
Consider 500mg aspirin 2x daily, a few days before & after the injection, & additional 500mg 1-2 hours before & after the injection.
Also perhaps increase your water intake, right before injection and for a week later, just not to obscene amounts
Also dipyridamol could help as prophylaxis against possible thrombocytopenia (as one of the anti-NETs/anti-coagulants out there).
[CONTRAINDICATIONS]
Dextromethorphan (robitussin)-increases viral replication
https://www.nature.com/articles/s41586-020-2286-9
Adrafinil/modafinil-releases histamine, which may worsen coronavirus inflammation
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2654794/
Azithromycin not helpful in mild-to-moderate cases
https://www.medrxiv.org/content/10.1101/2021.04.21.21255807v1
Ivermectin - currently as tested for safety as the vaccines.
A neurotoxin which may reveal its harmful properties with a blood-brain barrier-disrupting and blood-testis barrier-disrupting disease (like SARS-2) easily.
Currently no research is assessing any potential cognitive declines after its use despite the pre-print on SARS-CoV-2 S protein disrupting BBB being released as early as May 2020, with already countless media outlets covering the peer-reviewed version. For some reason, you will extremely rarely see anyone connecting the 2 basic dots.
>The quantitative analysis of adverse effects with Ivermectin use was inconclusive (OR 0.92, 95% CI 0.64-1.33; I2=14%).
https://www.medrxiv.org/content/10.1101/2021.04.30.21256415v1
https://archive.4plebs.org/pol/thread/298674728/#298697835
https://archive.4plebs.org/pol/thread/298674728/#298698824
https://archive.4plebs.org/pol/thread/298674728/#298699077
https://archive.4plebs.org/pol/thread/298674728/#298699491
https://archive.4plebs.org/pol/thread/298674728/#298702183
Ivermectin exhibits toxicity in testis and brain, if, correspondingly, blood-testis barrier and blood-brain barrier are breached or the P-glycoprotein responsible for preventing drug passage via the barriers is downregulated, or if the ivermectin dose is high enough, so that ivermectin bypasses the barriers.
Ivermectin impairs male fertility in rats when P-gp is inhibited
https://sci-hub.hkvisa.net/10.1016/j.etap.2008.03.011
Ivermectin impairs human fertility but unknown whether the dosage was that big or if the BTB was disrupted
https://www.scholarsresearchlibrary.com/articles/effects-of-ivermectin-therapy-on-the-sperm-functions-of-nigerian-onchocerciasis-patients.pdf
Neurotoxicity in human brains
>Clinical review of the cases within this case series has focused largely on [...] and evidence of secondary impairment of the blood-brain barrier.
>Obvious evidence of blood-brain barrier insufficiency, such as sepsis or malignancy, resulted in exclusion from the final case list
https://pdfs.semanticscholar.org/8a12/7da493b3fa9f9d28dca2b1f4201eebc811be.pdf
Problem is that SARS-CoV-2 disrupts the BBB (and may do same to BTB) via direct inflammatory damage or apoptosis, among other things
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7786155
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8112744
Also P-glycoprotein could be downregulated - via production of reactive oxygen species in mitochondria
https://archive.is/reBdL
[]
Or also inflammation
https://sites.ualberta.ca/~csps/JPPS7(3)/F.Gimenez/P-gp.htm
[]
Which is what SARS-2 would do
>Mounting evidence link the accelerated progression of the disease in COVID-19 patients to the hyper-inflammatory state termed as the “cytokine storm” involving major systemic perturbations. These include iron dysregulation manifested as hyperferritinemia associated with disease severity. Iron dysregulation induces reactive oxygen species (ROS) production and promotes oxidative stress. The mitochondria are the hub of cellular oxidative homeostasis.
https://www.sciencedirect.com/science/article/abs/pii/S1567724920301380
[]
Ivermectin could contribute to P-gp downregulation via those pathways btw
https://sci-hub.hkvisa.net/10.1016/j.bbrc.2016.10.064
As under-researched its safety is, and how many of better and safe alternatives there are known,
(nitric oxide nasal sprays)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8117664/
[]
(honey)
https://www.medrxiv.org/content/10.1101/2020.10.30.20217364v4.full
[]
(lactoferrin)
https://www.biorxiv.org/content/10.1101/2020.08.11.244996v4
[]
(etc)
ivermectin doesn't seem to be a good prophylaxis/treatment with efficacy that would really be worth the risks, especially when you consider how you'd have to keep taking it for a lifetime, as SARS-CoV-2 will keep being an endemic virus.
Remdesivir
Remdesivir may not cure coronavirus, but it’s on track to make billions for Gilead
>doctor at Seattle’s Harborview Medical Center: "We are continuing to use it, because if you look at all the data in total, there probably is some benefit.”
>probably
https://archive.vn/Q2djD
Anti-viral drug remdesivir has little to no effect on SARS-2 patients' chances of survival
https://www.bbc.com/news/world-54566730
Remdesivir does not improve clinical outcomes in people hospitalized with moderate pneumonia from SARS-2, a study published Friday by JAMA Network Open found
http://archive.is/AEy4A
https://jamanetwork.com/journals/jama/fullarticle/2769871
FDA expands use of SARS-2 treatment without research to back it up
>"It seems to be a pattern of approval without science, without data, without evidence," said Dr. Eric Topol, vice president for research at Scripps Research in La Jolla, California and a national expert on the use of data in medical research.
>In May, the FDA allowed remdesivir to be used for hospitalized patients who need oxygen, but not those sick enough to require ventilation. A government study published that month in the New England Journal of Medicine found those patients recovered faster than those who hadn't gotten the drug, though there was no evidence that it saved lives.
>No studies have been published since then supporting more widespread use of remdesivir, yet the FDA said the data is now compelling enough to expand its use.
https://archive.is/N9JWz
>The United States Army Medical Research Institute of Infectious Diseases + Fort Detrick's Sina Bavari was involved in helping Baric shill it
https://twitter.com/BillyBostickson/status/1292741360546508801
https://twitter.com/BillyBostickson/status/1293513471418499072
https://archive.4plebs.org/pol/thread/306304755/#306322283
In vitro evolution of Remdesivir resistance reveals genome plasticity of SARS-CoV-2
>Remdesivir (RDV) is used widely for COVID-19 patients despite varying results in recent clinical trials. Here, we show how serially passaging SARS-CoV-2 in vitro in the presence of RDV selected for drug-resistant viral populations. We determined that the E802D mutation in the RNA-dependent RNA polymerase was sufficient to confer decreased RDV sensitivity without affecting viral fitness. Analysis of more than 200,000 sequences of globally circulating SARS-CoV-2 variants show no evidence of widespread transmission of RDV-resistant mutants. Surprisingly, we also observed changes in the Spike (i.e., H69 E484, N501, H655) corresponding to mutations identified in emerging SARS-CoV-2 variants indicating that they can arise in vitro in the absence of immune selection.
https://www.biorxiv.org/content/10.1101/2021.02.01.429199v1
Convalescent plasma
Tocilizumab
Favipiravir (Favipavir)
Role of favipiravir in the treatment of adult patients with moderate to severe SARS-2: a single-center, prospective, observational, sequential cohort study from Hungary
>Favipiravir did not seem to affect disease progression. Further data are needed to position this drug among the anti-SARS-CoV-2 armamentarium.
https://www.medrxiv.org/content/10.1101/2020.11.26.20238014v1
https://pubmed.ncbi.nlm.nih.gov/33115675/
https://www.medrxiv.org/content/10.1101/2020.03.17.20037432v4
Toxicity/adverse events
>The Japanese study discussed previously found that adverse reactions were seen in around 20% of the patients who received favipiravir (at a dose lower than approved for COVID-19). The adverse effects were relatively minor and included hyperuricemia and diarrhea in 5% of the participants and reduced neutrophil count and transaminitis in 2% of the participants. One study showed occurrence of psychiatric symptoms in association with favipiravir. Effect of favipiravir in QTc prolongation is still uncertain, with some pharmacodynamic studies suggesting a positive association,24 but a Japanese study suggesting otherwise.
>Favipiravir use results in a dose-dependent increasing trend in the prevalence of hyperuricemia.24 A systematic review conducted by Pilkington et al. found similar trends across multiple studies.26 This is however not associated with clinical manifestations. There has been no evidence that hyperuricemia caused by favipiravir leads to clinical manifestations; however, longer follow-up periods would be required to fully assess this risk.
>There is evidence that favipiravir has a teratogenic potential and embryotoxicity. The Japanese drug safety bureau approval advises that favipiravir be given a strong warning against use in women of reproductive age and recommends precautionary statements on packaging and prescription alerts. The bureau also recommends that favipiravir should be avoided where alternative drugs could be used.24 Effective contraceptive methods during and for 7 days after the end of treatment need to be instructed to men who have received this treatment. Before favipiravir is prescribed to women of child-bearing age, it is imperative to rule out pregnancy with a negative urine pregnancy test.
https://archive.vn/aJPpj
Baloxavir Marboxil (Xofluza)
Clinical Outcomes and Plasma Concentrations of Baloxavir Marboxil and Favipiravir in COVID-19 Patients: An Exploratory Randomized, Controlled Trial
>Our findings could not prove a benefit of addition of either baloxavir marboxil or favipiravir under the trial dosages to the existing standard treatment
https://pubmed.ncbi.nlm.nih.gov/33115675/
HCQ - only good with zinc, and at low dosages
Low dose hydroxychloroquine is associated with lower mortality in SARS-2: a meta-analysis of 26 studies and 44,521 patients
>use of HCQ was associated with 21% lower mortality risk. This association vanished when daily dose >400 mg or total dose >4,400 mg were used, respectively.
https://www.medrxiv.org/content/10.1101/2020.11.01.20223958v1
You're risking with QTs prolongation and neurotoxicity, among other things, if you're using it for SARS-2
>Although the ability of HCQ to cross the blood-brain barrier (BBB) is not high (McChesney, 1983; Richardson et al., 2020), considering that HCQ has a very long half-life in vivo (Nirk et al., 2020), its direct effect on microglia should not be underestimated.
>In addition, HCQ may affect the CNS via its inhibitory effect on peripheral cytokines, such as IL-1β or TNF-α, which can bind to the vascular endothelium of the brain or directly entering the CNS (Jones and Thomsen, 2013), resulting in a reduction in the production of corresponding cerebral cytokines and induction of a neuroinflammatory deficit in the brain.
>Although hypo-neuroinflammation is not as concerning as hyper-neuroinflammation, and the latter has been indicated as a potential pathology of multiple psychiatric disorders (Bauer and Teixeira, 2019), emerging evidence suggests that maintaining the balance of the immune system is more important than preventing inflammation in the CNS (Magalhães et al., 2017) and that low levels of inflammation in the brain can also have negative effects on cognition and behaviors (Graeber, 2010; Zhang et al., 2019).
>immunosuppressive effect of HCQ may have negative effects on the CNS, especially in healthy individuals who do not suffer from hyperinflammation induced by infection.
https://www.frontiersin.org/articles/10.3389/fphar.2021.633112/full
>Baseline average automated QTc was 415 ± 29 ms and lengthened to 438 ± 40 ms after 48 hours of combined therapy. The treatment had to be stopped because of significant QTc prolongation in two out of 71 patients (2.8%)
https://pubmed.ncbi.nlm.nih.gov/32588427
https://pubmed.ncbi.nlm.nih.gov/32610165
*************************************************************************************************
Much thanks to anons in /cvg/, anonymous author of the original list
>https://pastebin.com/QCJEsu41
and the other anonymous author of
>https://pastebin.com/raw/3MMpRP54
for breaking the initial ground of this